Author: Gajo Nicolas MD *1, Baroudi Errouane MD 2, Damak Hassen MD 3
Author Affiliation:
1 Assistant Physician, Emergency Department, Jura Hospital, Delémont, Switzerland.
2 Head Physician, Emergency Department, Jura Hospital, Delémont, Switzerland.
3 Senior Physician, Emergency Department, Jura Hospital, Delémont, Switzerland.
Competing Interests: The author/s declare no competing interests.
Issue: 16.03
DOI: 10.30756/ahmj.2025.16.03
Received: Sept 25, 2025
Accepted: Dec 18, 2025
Published: Dec 29, 2025
Recommended Citation: Nicolas G, Errouane B, Hassen D. Transient Perivascular Inflammation Of The Carotid Artery (TIPIC) Syndrome. Ann Head Med. 2025;16:03. DOI: 10.30756/ahmj.2025.16.03
Introduction
The Transient Perivascular Inflammation of the Carotid Artery (TIPIC) syndrome is a rare clinical entity, leading to tenderness and acute pain at the carotid bifurcation without an identifiable cause 1, 2. First described by Fay in 1927 3 and later by Roseman in 1967 4, it was formerly known as Fay syndrome or idiopathic carotidynia/carotidodynia 3-5. TIPIC syndrome is a benign condition with a favorable course, and its diagnosis is based on clinical presentation coupled with radiological findings 1, 2, 6.
Case Report
We report the case of a 40-year-old woman, mother of five living children, with a medical history of arterial hypertension (treated with hydrochlorothiazide 25 mg), atrial fibrillation (treated with rivaroxaban 20 mg and metoprolol LP 25 mg), pollen allergy, cholecystectomy in 2016, and a spontaneous miscarriage in 2005. She presented to the emergency department in 2023 with a 3-day history of left anterior cervical pain. Since 2014, she had visited the emergency department four times for headaches, one of which resembled the current episode. During one of these visits, a contrast-enhanced cranial CT scan ruled out hemorrhage and venous thrombosis. On each occasion, a diagnosis of tension-type headache was made, and the patient was discharged with analgesic treatment.
During the current consultation, the medical history revealed spontaneous, pulsatile pain in the left anterior neck, exacerbated by head movements, particularly toward the left, and radiating to the head and ipsilateral face. The pain was relieved by acetaminophen. The patient reported no other symptoms, including fever, chills, weight loss, or ENT, neurological, or respiratory complaints). There was no recent travel animal contact, or risk factors for sexually transmitted infections.
Vital signs, including respiratory, hemodynamic, and neurological parameters were within normal limits. Neck examination revealed a tender, pulsatile, soft, well-defined left-sided mass, mobile relative to underlying structures, measuring approximately 0.5 x 1 cm. No overlying skin inflammation, lesions, or vascular murmurs were observed. Neurological examination was normal, lymph node areas were unremarkable, and no other clinical abnormalities were identified.
Blood analyses were within normal limits, showing no signs of inflammation (Haemoglobin 118 g/L, Leucocytes 9.8 G/l, Thrombocytes 339 G/l, CRP 14.3 mg/l, Natrium 138 mmol/l, Kalium 3.7 mmol/l, Creatinine 45 umol/l, MDRD>60 ml/min/1.73m2, Urea 3.9 mmol/l)
A Doppler ultrasound of the soft tissues revealed an eccentric thickening of the carotid bulb wall, suggestive of a carotid dissection (Figures 1 & 2). This finding prompted a CT scan.
The contrast-enhanced neck CT scan ruled out carotid dissection. The findings observed on ultrasound was interpreted as carotid wall thickening with possible thrombosis and signs of recanalization (Figures 3, 4, & 5), indicating the need for an MRI to confirm (further refine and confirm) the diagnosis.


The cervical MRI, performed with and without contrast, ruled out both dissection and carotid artery thrombosis but revealed a poorly defined mass on the non-contrast sequences (Figures 7 & 8). After Gadolinium injection, a left peri carotid infiltrate was observed. (Figures 9 &10).

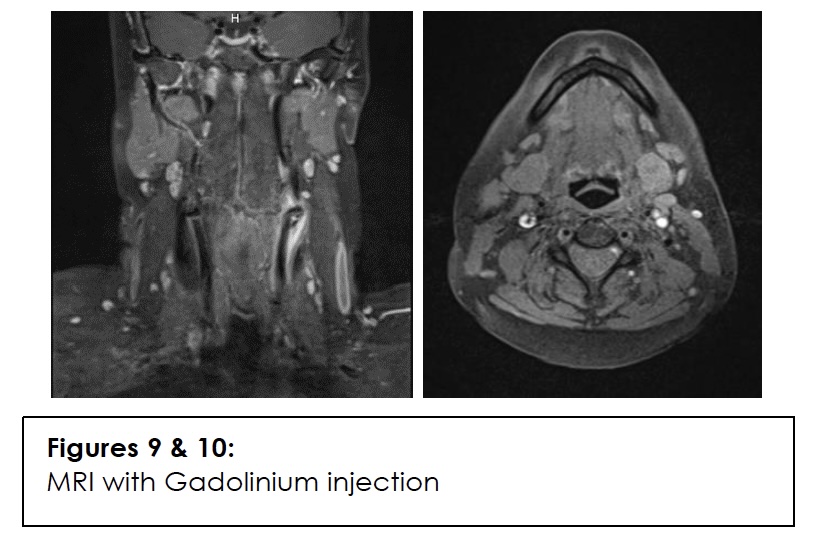
The diagnosis of Transient Perivascular Inflammation of the Carotid Artery (TIPIC) syndrome was confirmed. The patient was discharged with symptomatic treatment consisting of Ibuprofen (400 mg three times daily for 5 days) and acetaminophen (1 g four times daily for 3 days).
Follow-up in the emergency department after 7 days showed complete resolution of symptoms. Given this rapid improvement, the patient declined further ultrasound imaging and chose to continue follow-up with her general practitioner.
Discussion
TIPIC is a transient perivascular inflammation of the carotid artery, resulting in tenderness and acute pain at the carotid bifurcation 1, 7. In 1988, the syndrome was included in the first international classification of headaches by the Headache Classification Committee of the International Headache Society 8. However, in 2004, it was removed due to imprecise diagnostic criteria 9, 10. Subsequent advances in imaging have demonstrated abnormalities of the carotid wall and surrounding soft tissues, particularly near the bifurcation, in the absence of any identifiable alternative cause. These findings have led to the development of clearer and more rigorous diagnostic criteria, establishing TIPIC as a clinic-radiological entity 1, 6, 11. The acronym TIPIC was adopted in 2017 following a multidisciplinary consensus and a retrospective study involving 47 patients 11.
TIPIC is considered rare, with a reported prevalence of 2.8% among patients presenting with acute cervical pain 11, 12. However, this condition is likely underrecognized, as its nonspecific symptoms and tendency for spontaneous resolution often leads to misdiagnosis. 1, 11, 13. A slight female predominance has been noted (ratio 1.1-1.5:1), with a mean age of approximately 37 years 7, 12.
Clinically, although the presentation is often nonspecific, it can nonetheless be suggestive, as illustrated by our patient’s case. The pain is typically acute, peri carotid, moderate in intensity (approximately 5/10), and occurs without an identifiable trigger. It is unilateral in about 90% of cases and bilateral in 4–10%. The pain frequently radiates toward the ipsilateral ear, face, and head. In some patients, it is exacerbated by swallowing, chewing, neck movement, coughing, yawning, or sneezing 1, 2, 6, 7, 12, 14-20. Clinical examination almost always reveals tenderness over the carotid artery, particularly at the bifurcation, and palpation often elicits a painful, pulsatile mass. Neurological signs are reported in approximately 17% of cases and should prompt urgent evaluation for a possible cerebrovascular cause, such as acute stroke. Documented neurological manifestations include dizziness, paraesthesia or allodynia, dysesthesia, peripheral facial palsy, or ipsilateral paraesthesia. These symptoms, like the cervical pain, typically resolve spontaneously 1, 2, 7, 12, 21-25. Some reports have suggested potential triggers, including stress, bright light, loud sounds, menstruation, and tobacco use 17, 26.
Laboratory testing is primarily useful for excluding alternative diagnoses, as no specific biological marker for TIPIC has been identified. In most cases, laboratory parameters remain within normal limits. Nonetheless, some studies have reported abnormalities, including inflammatory syndrome with elevated ESR (erythrocyte sedimentation rate) and/or CRP (C-reactive protein) in approximately 6% of patients, increased serum amyloid A, and elevated vasculitis-associated markers such as soluble intracellular adhesion molecule-1 (sICAM-1) 2, 6, 7, 12, 20, 25, 27-30.
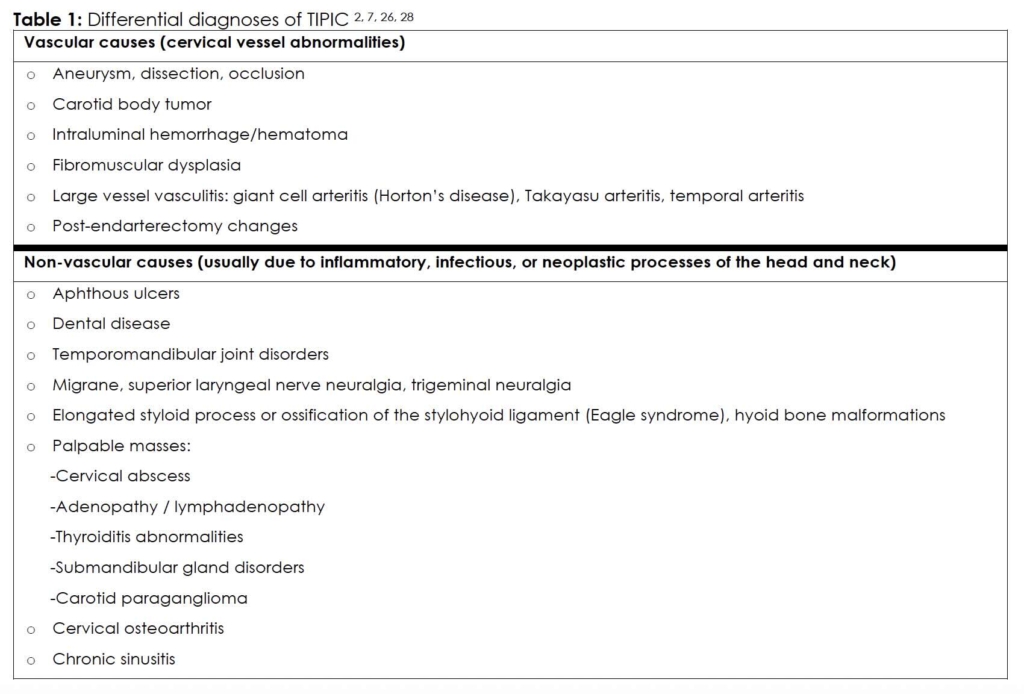
TIPIC remains a diagnosis of exclusion; therefore, serious alternative conditions necessitating urgent management must be ruled out beforehand 2, 7, 26, 28 (Table 1).
Since the early 21st century, advances in the quality and sensitivity of medical imaging have enabled the diagnosis of TIPIC in patients with suggestive clinical presentations, while simultaneously excluding more urgent and serious differential diagnoses 11, 26.
Ultrasound of the neck soft tissues and Doppler ultrasound of the supra-aortic trunks can reveal several characteristic patterns:
- Patent carotid arteries without significant atheromatous deposits. There is clear thickening of the posterior wall of the carotid bifurcation, extending from the bulb to the ostia of the internal and external carotid arteries, without any hemodynamic impact 1, 6, 9
- Hypoechoic appearance of the wall and intima at the common-to-internal carotid junction, potentially suggesting either a soft plaque or a localized inflammatory thickening, without any hemodynamic consequences 1, 6, 31
- Perivascular changes measuring 4–5 mm in thickness and 15–28 mm in length 17, 31
- Diffuse hypoechoic infiltration around the carotid bifurcation, eliciting pain upon probe palpation 7
- Lesions are predominantly located posteriorly and laterally to the carotid bifurcation 1
- Wall thickening can moderately narrow the lumen in approximately 38% of cases, without affecting flow¹¹. However, significant stenosis has been reported in 6% of according to literature reviews 1
CT and CT angiography of the neck confirms asymmetry in the carotid bulb diameter, with an ill-defined lesion surrounding the bifurcation due to regular hypodense wall thickening in its posterior aspect. This appearance may mimic stenosis and may demonstrate peripheral enhancement in delayed phases 7, 8, 18.
MRI confirms wall thickening with infiltration of the adjacent soft tissues, particularly posterior and medial to the bifurcation. This appears as contrast enhancement on T1-weighted sequences with fat suppression, and as hyperintensity on T2-weighted, consistent with perivascular inflammation. The characteristic morphology helps differentiate TIPIC from soft-tissue tumors 1, 32, 33.
MRI also demonstrates diffuse, ill-defined thickening around the bifurcation, extending along the internal carotid artery. The lesion is hyperintense on T2-weighred sequences and exhibits marked enhancement after gadolinium injection, consistent with peri-adventitial inflammatory tissue 7, 26, 32, 33.
Imaging criteria are specific:
- Constant finding: eccentric perivascular infiltration of the carotid bulb, detectable on both ultrasound and MRI 12, 13, 31-33.
- Ultrasound: hypoechoic thickening of the vessel wall 1, 6, 31.
- Cervical MRI: isointense lesion on T1-weighted sequences with fat saturation, hyperintense on T2-weighted sequences, showing strong focal and perivascular contrast enhancement after Gadolinium injection 12, 32, 33.
- Ultrasound remains superior to MRI for diagnosis due to its high resolution, non-invasiveness, and accessibility 12, 32, 33.
In 2004, the International Headache Society proposed diagnostic criteria 9, and in 2017, Lecler et al. 11 provided a detailed clinico-radiological description of the condition. The currently accepted diagnostic criteria include 1, 2, 6, 7, 10, 30, 34:
- Unilateral neck pain over the carotid artery, potentially radiating to the face.
- Presence of at least one of the following signs in the carotid region: tenderness, swelling, or increased pulsation.
- Pain triggered by palpation of the carotid bifurcation.
- Characteristic imaging findings: perivascular thickening without wall or intraluminal abnormalities, and exclusion of alternative diagnoses.
- No other etiology identified after appropriate investigations.
- Good response to NSAIDs or spontaneous resolution within approximately two weeks
Therefore, in the absence of alternative aetiologies, TIPIC syndrome can be diagnosed—as in our patient—when a suggestive clinical presentation is accompanied by localized perivascular inflammatory infiltration on imaging.
In patients with suggestive clinical presentation and compatible imaging, biopsy and histopathological analysis are generally unnecessary for the diagnosis or management of TIPIC 29. When performed, macroscopic examinations typically reveal a greyish carotid artery, occasionally exhibiting oedema. Histology demonstrated an acute-to-chronic inflammatory process with polymorphic cellular proliferation predominantly lymphocytes and fibroblasts, along with scattered neutrophils, mast cells, and eosinophils. The hallmark feature is proliferation of small vessels within a fibro-myxoid stroma, which is distinct from granulation tissue, abscess, or vasculitis, and is notably devoid of giant cells 7, 27, 28.
In typical cases, the clinical course is usually benign, with spontaneous regression or improvement under anti-inflammatory treatment within 10-14 days. Follow-up MRI usually demonstrates partial or complete resolution of the inflammatory process 1, 7. In atypical cases, however, radiologic anomalies may persist despite clinical symptoms resolution, including fibrous plaques in the carotid bulb, indicative of early fibrosis associated with low-grade chronic inflammation, observed 2-3 months after the acute episode 1, 11, 35. Furthermore, TIPIC syndrome has been proposed as a potential risk factor for the development of atherosclerotic plaques secondary to arterial wall inflammation, warranting prolonged patient surveillance 11, 13, 25. Recurrence can occur in 10-19% of patients within 1-6 months 1, 25.
Treatment of TIPIC syndrome is primarily symptomatic and relies on nonsteroidal anti-inflammatory drugs (NSAIDs) or corticosteroids. No comparative studies evaluating efficacy have been conducted. Although some authors have reported the use of pizotifen, methysergide, or propranolol, these approaches remain without consensus 2, 26, 35, 36.
Conclusion
TIPIC syndrome is a benign but poorly recognized entity that is likely under-diagnosed. Often idiopathic, its diagnosis relies on anamnesis, clinical findings, and imaging primarily ultrasound and MRI. Nevertheless, it remains a diagnosis of exclusion, occasionally necessitating the exclusion of other conditions requiring urgent medical management. Treatment is symptomatic, and the clinical course is favorable, although relapses can occur, albeit rarely.
References
- J.-B. Brunet de Courssou CO, S. Madec, M.-N. De La Lance, C. Doutrelon, I. Taifas. Transient perivascular inflammation of the carotid artery (TIPIC) syndrome: Two case reports with overview of the literature. Pratique Neurologique – FMC. 2022;13(3):188-194. doi:10.1016/j.praneu.2022.07.007
- Takamura A, Hori A. Recurrent TransIent Perivascular Inflammation of the Carotid artery syndrome with temporary carotid plaque on ultrasonography: a case report. Clin Case Rep. Nov 2017;5(11):1847-1851. PubMed PMID: 29152284; PubMed Central PMCID: PMCPMC5676270. doi:10.1002/ccr3.1209
- Fay T. Atypical neuralgia. Arch Neurol Psychiatry. 1927;18:309–15.
- Roseman DM. Carotidynia. A distinct syndrome. Arch Otolaryngol. Jan 1967;85(1):81-4. PubMed PMID: 6016255. doi:10.1001/archotol.1967.00760040083016
- Fay T. Atypical neuralgia: a pain syndrome of vascular pain. Annals of Otology, Rhinology & Laryngology. 1932;41:1030-1062.
- Maggialetti N, De Marco I, Sasso S, et al. “TransIent perivascular inflammation of the carotid artery (TIPIC) syndrome” as a rare case of laterocervical pain: Multimodal diagnosis. Radiol Case Rep. Jul 2022;17(7):2378-2382. PubMed PMID: 35570872; PubMed Central PMCID: PMCPMC9096471. doi:10.1016/j.radcr.2022.04.021
- Dulguerov P, Kohler R, Becker M. [Carotidynia and Eagle syndrome: two neck pain syndromes to be rediscovered]. Rev Med Suisse. Oct 5 2011;7(311):1929-34. Carotidynie et syndrome d’Eagle: deux syndromes classiques a redecouvrir. PubMed PMID: 22046682.
- Society HCSotIH. Classification and diagnostic criteria for headache disorders, cranial neuralgias and facial pain. Cephalalgia. 1988;8(Suppl 7):1-96.
- Headache Classification Subcommittee of the International Headache S. The International Classification of Headache Disorders: 2nd edition. Cephalalgia. 2004;24 Suppl 1:9-160. PubMed PMID: 14979299. doi:10.1111/j.1468-2982.2003.00824.x
- Korbecka J, Chojdak-Lukasiewicz J, Sulima K, Korbecki A, Bladowska J, Paradowski B. Transient perivascular inflammation of the carotid artery syndrome as a rare cause of unilateral neck pain. Pol Arch Intern Med. Aug 30 2023;133(7-8)PubMed PMID: 37405685. doi:10.20452/pamw.16525
- Lecler A, Obadia M, Savatovsky J, et al. TIPIC Syndrome: Beyond the Myth of Carotidynia, a New Distinct Unclassified Entity. AJNR Am J Neuroradiol. Jul 2017;38(7):1391-1398. PubMed PMID: 28495942; PubMed Central PMCID: PMCPMC7959891. doi:10.3174/ajnr.A5214
- Badou E, Lecler A, Veyrat M, El Bakkouri W. TransIent Perivascular In fl ammation of the Carotid artery syndrome: TIPIC, a new clinical entity that must be recognised by ENT surgeons. Eur Ann Otorhinolaryngol Head Neck Dis. Jan 2020;137(1):87-88. PubMed PMID: 31836495. doi:10.1016/j.anorl.2019.10.001
- Abrahamy M, Werner M, Gottlieb P, Strauss S. Ultrasound for the Diagnosis of Carotidynia. J Ultrasound Med. Dec 2017;36(12):2605-2609. PubMed PMID: 28708261. doi:10.1002/jum.14321
- Chen XW, Li J, Ren CP, Jiao Y. Unilateral neck pain and headache, vocal hoarseness, swallowing difficulty, and fainting attacks: a case report of idiopathic carotidynia with unusual clinical manifestations. Chin Med J (Engl). Oct 5 2019;132(19):2392-2394. PubMed PMID: 31567387; PubMed Central PMCID: PMCPMC6819046. doi:10.1097/CM9.0000000000000466
- Arnould B, Miranda S, Mignon F, Camus V. G-CSF-induced TIPIC syndrome and large vessel vasculitis: A case report. Clin Case Rep. Sep 2023;11(9):e7918. PubMed PMID: 37720704; PubMed Central PMCID: PMCPMC10502199. doi:10.1002/ccr3.7918
- Ulmer TP, Kraus CK. A pain in the neck. J Am Coll Emerg Physicians Open. Jun 2023;4(3):e12973. PubMed PMID: 37223214; PubMed Central PMCID: PMCPMC10202195. doi:10.1002/emp2.12973
- Micieli E, Voci D, Mumoli N, et al. Transient perivascular inflammation of the carotid artery (TIPIC) syndrome. Vasa. Mar 2022;51(2):71-77. PubMed PMID: 35130715. doi:10.1024/0301-1526/a000989
- Modi T, Verma M, Ahuja G, Kamat N, Patkar DP. TIPIC-A Newly Recognized Syndrome: Multimodality Imaging of a Rare Clinicoradiological Entity. Indian J Radiol Imaging. Apr 2021;31(2):488-491. PubMed PMID: 34556937; PubMed Central PMCID: PMCPMC8448226. doi:10.1055/s-0041-1734353
- Hersh SP, Gerard P, Hersh J. Carotidynia Versus Transient Perivascular Inflammation of the Carotid Artery (TIPIC) Syndrome: Finding Common Ground. Cureus. Sep 2021;13(9):e17684. PubMed PMID: 34650859; PubMed Central PMCID: PMCPMC8487627. doi:10.7759/cureus.17684
- Venetis E, Konopnicki D, Jissendi Tchofo P. Multimodal imaging features of transient perivascular inflammation of the carotid artery (TIPIC) syndrome in a patient with Covid-19. Radiol Case Rep. Mar 2022;17(3):902-906. PubMed PMID: 35043074; PubMed Central PMCID: PMCPMC8758192. doi:10.1016/j.radcr.2021.12.005
- Nishizawa T, Uematsu H. Transient perivascular inflammation of the carotid artery syndrome. BMJ Case Rep. Jan 4 2022;15(1)PubMed PMID: 34983814; PubMed Central PMCID: PMCPMC8728453. doi:10.1136/bcr-2021-248637
- Ganesan P, Durai I. Multimodality imaging of transient perivascular inflammation of carotid artery (TIPIC) syndrome: a case report. Egyptian Journal of Radiology and Nuclear Medicine. 2023/09/25 2023;54(1):162. doi:10.1186/s43055-023-01113-x
- Holay Q, Hak JF, Varoquaux A. Transient Perivascular Inflammation of the Carotid Artery (TIPIC) Syndrome: An Uncommon Cause of Anterior Neck Pain. Pain Med. Jan 3 2022;23(1):212-213. PubMed PMID: 34550372. doi:10.1093/pm/pnab286
- Jud P, Kangler G, Gressenberger P, Portugaller RH, Brodmann M. Images of the month 3: Transient perivascular inflammation of the carotid artery syndrome. Clin Med (Lond). Jul 2021;21(4):e412-e413. PubMed PMID: 35192487; PubMed Central PMCID: PMCPMC8313193. doi:10.7861/clinmed.2021-0349
- Baverez C, Berthoux E, Pérard L. Une maladie TIPIC : à propos de 3 cas. La Revue de Médecine Interne. 2021/06/01/ 2021;42:A162. doi:https://doi.org/10.1016/j.revmed.2021.03.144
- Murray TJ. Carotidynia: a cause of neck and face pain. Can Med Assoc J. Feb 17 1979;120(4):441-3. PubMed PMID: 445285; PubMed Central PMCID: PMCPMC1818881.
- Santarosa C, Stefanelli S, Sztajzel R, Mundada P, Becker M. Carotidynia: A Rare Diagnosis for Unilateral Neck Pain Revealed by Cross-Sectional Imaging. Case Rep Radiol. 2017;2017:7086854. PubMed PMID: 29147596; PubMed Central PMCID: PMCPMC5632850. doi:10.1155/2017/7086854
- da Rocha AJ, Tokura EH, Romualdo AP, Fatio M, Gama HP. Imaging contribution for the diagnosis of carotidynia. J Headache Pain. Apr 2009;10(2):125-7. PubMed PMID: 19198982; PubMed Central PMCID: PMCPMC3451642. doi:10.1007/s10194-009-0099-1
- Cassone G, Colaci M, Giuggioli D, Manfredi A, Sebastiani M, Ferri C. Carotidynia Possibly due to Localized Vasculitis in a Patient with Latent Mycobacterium tuberculosis Infection. Case Rep Vasc Med. 2013;2013:585789. PubMed PMID: 24363952; PubMed Central PMCID: PMCPMC3864074. doi:10.1155/2013/585789
- Mathangasinghe Y, Karunarathne RU, Liyanage UA. Transient perivascular inflammation of the carotid artery; a rare cause of intense neck pain. BJR Case Rep. Dec 2019;5(4):20190014. PubMed PMID: 31938559; PubMed Central PMCID: PMCPMC6945257. doi:10.1259/bjrcr.20190014
- Rafailidis V, Chryssogonidis I, Tegos T, Partovi S, Charitanti-Kouridou A, Staub D. Role of multi-parametric ultrasound in transient perivascular inflammation of the carotid artery syndrome. Ultrasound. May 2019;27(2):77-84. PubMed PMID:
Consent
Consent was obtained from the patient for the publication of this case report, including all relevant clinical information and imaging.
Declarations/Disclosures
Funding/Conflicts of interest: In compliance with the ICMJE uniform disclosure form, author declares the following:
Payment/services info: Author has declared that no financial support was received from any organization for the submitted work.
Financial relationships: Author have declared that they have no financial relationships at present or within the previous three years with any organizations that might have an interest in the submitted work.
Other relationships: Author have declared that there are no other relationships or activities that could appear to have influenced the submitted work.