Author: Adlai Pappy II MD, MBA *1, Kathryn Satko BA, MA 1, Alexandra Savinkina MSPH 2, Jenny Yau BS 3, Linda N. Lee MD, FACS 3, Robert J. Yong MD, MBA 1
Author Affiliation:
1 Brigham and Women’s Hospital, Department of Anesthesiology, Critical Care, and Pain Medicine, Boston, MA.
2 Department of Epidemiology of Microbial Diseases, Yale School of Public Health, New Haven, CT, USA; Public Health Modeling Unit, Yale School of Public Health, New Haven, CT.
3 Department of Otolaryngology, Division of Facial Plastic & Reconstructive Surgery, Massachusetts Eye and Ear, Harvard Medical School, 243 Charles St, Boston, MA 02114.
Competing Interests: The author/s declare no competing interests.
Issue: 15.02
DOI: 10.30756/ahmj.2025.15.02
Received: May 12, 2025
Accepted: Jul 7, 2025
Published: Jul 25, 2025
Recommended Citation: Pappy A, Satko K, Savinkina A, Yau J, etal Health Utility In Chronic Migraine Sufferers: Assessing Quality Adjusted Life-Years. Ann Head Med. 2025;15:02. DOI: 10.30756/ahmj.2025.15.02
Chronic migraine is a common neurologic disorder posing a significant economic burden from absenteeism and medical treatments. Despite chronic migraine’s significant impact, no studies have directly aimed to survey these individuals to quantify their disease burden using validated health utility measures. Our study aims to quantify the significance of their disease burden.
The survey utilizes the Standard Gamble (SG), Time Trade-Off (TTO), and Visual Analog Scale (VAS) measures to quantify the health utility states of those with chronic migraine to determine Quality-Adjusted Life-Years (QALY). Monocular and binocular blindness health utility scores were used as controls for the study.
A total of 39 patients with migraine were included in this study. Patients who indicated that monocular blindness had worse health utility than binocular blindness were removed from the data as a screening control. A total of 29 patients passed the survey control screen. When comparing VAS, SG, and TTO utility scores for monocular blindness to chronic migraine, patients’ utility scores for chronic migraine were statistically significantly worse than those for monocular blindness by an average of 21.6% across all three utility scores (p ≤ 0.01). This study is the first to systematically survey patients with chronic migraine to present descriptive statistics that highlight the significant negative impact of chronic migraine on health utility.
Introduction
Several studies have examined the quality of life in patients with acute or chronic debilitating pain and the psychological effects of it. However, few studies to date have quantified the health state utility of chronic migraine1. Migraine is a common neurologic disorder, with close to 6% of men and 18% of women in the United States suffering from this disease2. The pain can be severe and occur many times during any given month for a patient3. Additionally, its peak prevalence occurs in patients’ most productive years, ranging from 25 to 55 years of age4. This results in a large economic burden that occurs with direct healthcare costs averaging £2,579 to £48,810 (GBP 2021) per patient and indirectly with absenteeism and other costs averaging £1,754.52 to £8,219.46 per patient5, 6. Despite advances in treatments over the years, there remains a large portion of the patient population who are refractory to these medications.
Therefore, this study employs validated survey tools to determine the disease burden for chronic migraine patients, comparing the health utility scores of chronic migraines with those of their respective age groups. Evaluation of the health state utility of chronic migraine as assessed by chronic migraine patients will help in the commissioning of appropriate medical care and treatment, developing local and regional services, and creating novel therapies to adequately treat these individuals.
The primary aim of this study is to quantify the health utility states of people who experienced chronic migraine as a descriptive measure to aid health economists who are working to determine a Quality-Adjusted Life-Years (QALY) for various applications to compare and determine value quantitatively. This collective information can be used to tailor individual chronic migraine treatments to improve the quality of life and adequately treat pain symptoms among patients receiving peripheral nerve blocks, onabotulinumtoxinA, or other interventional or medication management.
Methods
Patients
Inclusion criteria included patients diagnosed with chronic migraine by a healthcare professional according to the International Classification of Headache Disorders (ICHD) 3rd edition7. Participants were required to be between 18 and 89 years of age at enrollment. Patients diagnosed with chronic migraine were contacted after expressing interest in completing the survey. The study survey was conducted as a prospective observational study design. Study data were collected and managed using Research Electronic Data Capture (REDCap) electronic data capture tools hosted at Harvard University8, 9. REDCap is a secure, web-based software platform designed to support data capture for research studies.
Health Utility Survey
The survey utilizes three validated health utility measures. The Standard Gamble (SG) assesses patient preferences by presenting a choice between living with a health condition versus taking a gamble with a chance of perfect health or death. The Time Trade-Off (TTO) measures how many years of life in perfect health a patient would consider equivalent to a longer period living with their current condition. The Visual Analog Scale (VAS) uses a 0-100 scale where patients rate their current health state with 0 representing death and 100 representing perfect health. These three measures were used to quantify the health utility states of those with chronic migraine. Each health state had an associated vignette state that was developed from patient encounters documented in our chronic pain clinic. This study design is validated for descriptive statistics since chronic migraine patients were asked to rate these states in a stated-preference experiment that utilized TTO, SG, and VAS pain scores to determine QALY10. In addition to taking QALY, TTO, and SG questions as part of a health utility survey, patients were asked to take an EuroQol 5-dimension 5-level (EQ-5D-5L) survey to assess general health11, 12. The EQ-5D-5L is a health assessment tool that measures quality of life across five dimensions (mobility, self-care, usual activities, pain/discomfort, and anxiety/depression) with five response levels each, ranging from “no problems” to “extreme problems,” used to produce health utility scores for economic evaluations, research comparisons, and healthcare decision-making. No immediate benefit was awarded to study participants to prevent bias. For this reason, the exclusion of children from study participation does not withhold any perceived benefit, as no such immediate benefit exists. The Mass General Brigham Institutional Review Board approved the protocol (Protocol number 2022P00632).
Analysis
Monocular and binocular blindness utility using the VAS, SG, or TTO was used as a control to identify patients who did not provide quality answers. These are accepted controls for these types of surveys used to assess patient health utility. Patients who provided identical responses across each of these scenarios or indicated a worse disease burden for monocular blindness were considered to have poor survey comprehension. This is considered poor comprehension because the assumption was made that a person completing the survey should always consider the disease burden of binocular blindness worse than that of monocular blindness. Their responses were deemed unreliable and were excluded from the data analysis. Thus, they were excluded from the data analysis. Of the 39 patients who completed the survey, ten (25.6%) were excluded from the analysis.
Data were assessed with a t-test comparison to detect whether any significant differences existed among VAS, SG, and TTO scores between each health state. Pairwise significance was adjusted using the Bonferroni correction to reduce the chance of type I error for multiple comparisons. Results were considered significant if p ≤ 0.05 was observed. Statistical analyses were completed using Excel and R software. Means and standard deviations (SD) of utility scores were calculated and normalized to a continuous 0 to 1 scale.
Results
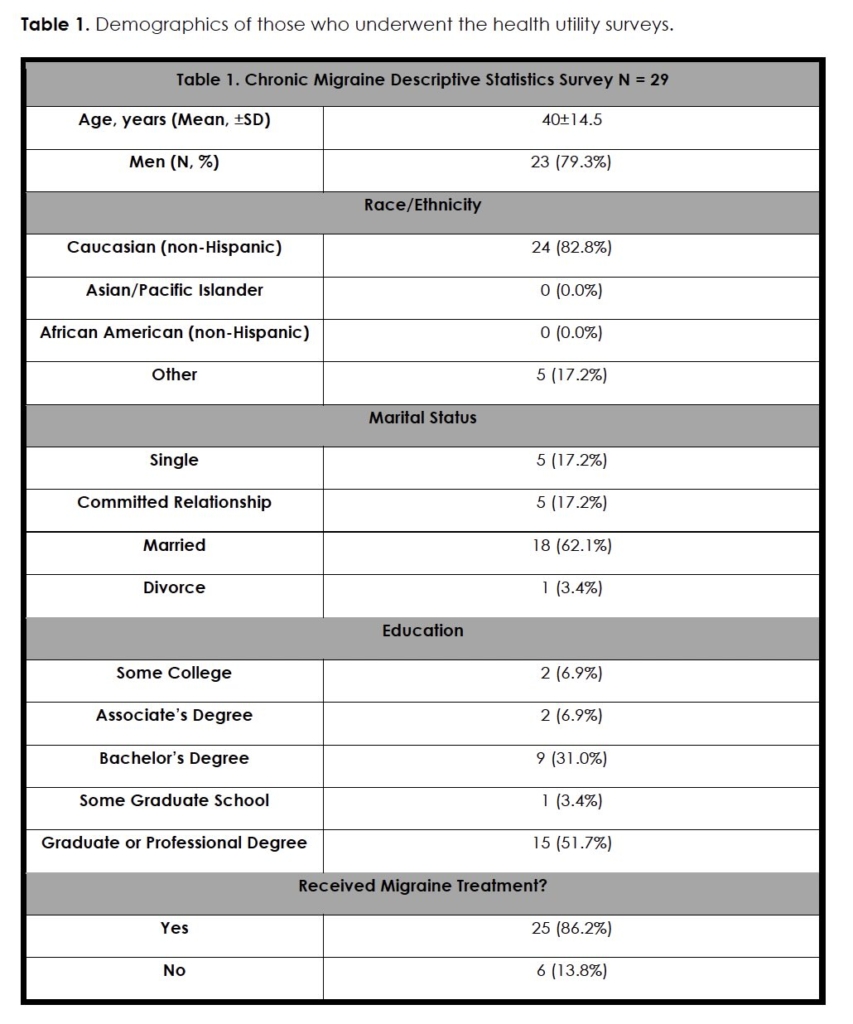
A total of 39 patients with migraine underwent the survey. Ten patients were excluded from the analysis due to failing to pass the monocular and binocular blindness control. Of the 29 included in the analysis, 23 (79.3%) were male, and 6 (20.7%) were female. The mean age of participants was (40.0 years ± 14.5) (Table 1). Most female and male participants were under the age of 50, making up 67.7% and 87.5% of each gender, respectively. There were no statistically significant differences in age distribution between female and male participants (p = 0.46). Of the participants, 62.1% were married. Most of the participants had an undergraduate, graduate, or professional degree (82.8%). Marital status did not differ significantly between female and male participants (p = 0.14). Additionally, 24 of the participants were Caucasian (82.8%), which was the vast majority of the participants. There were no statistically significant differences in the demographics of those who were surveyed. Of the survey takers, 25 had received treatment for their migraine (86.2%).
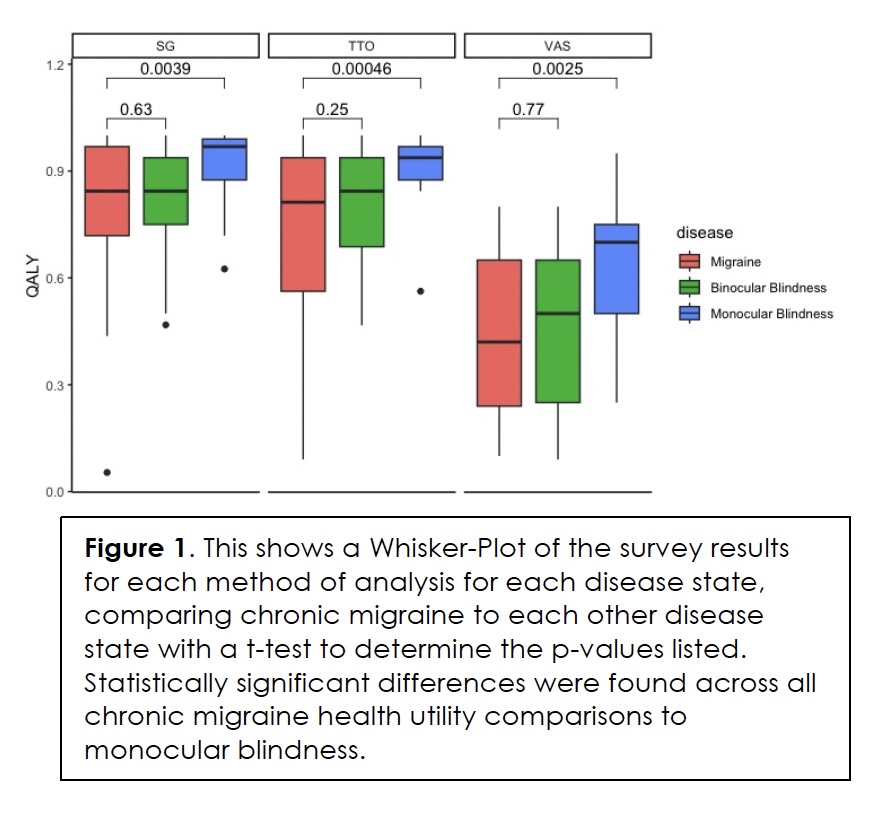
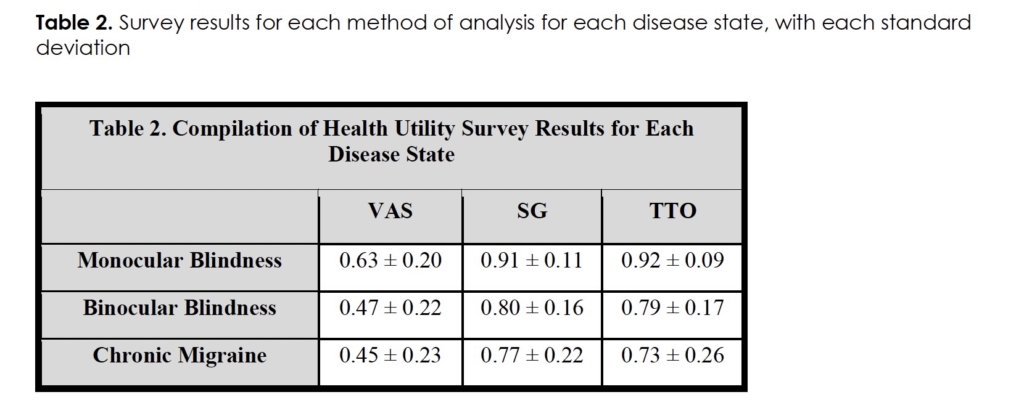
The QALY was assessed from the perspective of chronic migraine patients for the disease states of chronic migraine, monocular blindness, and binocular blindness. The descriptive statistics of the QALY for VAS, SG, and TTO assessments are depicted in Table 2. When comparing VAS, SG, and TTO utility scores for chronic migraine (0.45±0.23, 0.77±0.22, 0.73±0.26, respectively) and monocular blindness (0.63±0.2, 0.91±0.11, 0.92±0.09, respectively), patients’ VAS, SG, and TTO utility scores for chronic migraine were statistically significantly worse than monocular blindness by an average of 21.6% across all three utility scores (p ≤ 0.01). For VAS, SG, and TTO utility scores for chronic migraine compared to binocular blindness (0.47±0.22, 0.80±0.16, 0.79±0.17, respectively) trended towards worse disease burden for chronic migraine, but these health utility scores showed no statistically significant difference. These tabular differences are also shown in a Whisker-Plot for each method of analysis for each disease state to further depict the aforementioned results (Figure 1).
Discussion
This study is the first to directly assess the significance of chronic migraine disease burden, specifically in patients suffering from this disease, in contrast to surveys that are a baseline assessment for clinical trial enrollment. The results compared to other diagnoses for which we have descriptive data highlight the significance of chronic migraine as a disease. The evidence for the significance of disease burden is clear when comparing the controls of monocular blindness to chronic migraine, which showed chronic migraine to be statistically significantly worse than monocular blindness (p ≤ 0.01) across our three health utility scoring modalities. The finding that chronic migraine patients prioritize resolving chronic migraine over the resolution of monocular blindness is clinically meaningful. These results support the paramount need for timely diagnosis, treatment, and research funding into further treatments for this chronic disease.
Other studies in the literature have used SG, TTO, and VAS to show, through assumption, the financial significance of treatment for other disease states13. For our study, we can utilize the following assumptions to quantify the disease burden in dollars and provide an example of the significance. Given that TTO utilizes 36 years lived, it was assumed that resolution of symptoms would, at a minimum, improve our patients’ utility score to the average for the United States of 0.82 for the age range of 65 – 74. This would be an increase in utility state of 0.09 and would comprise a cost-effective threshold of at least $324,000 at a willingness-to-pay threshold of $100,000 per QALY. Additionally, the difference in QALY values suggests that chronic migraine patients lose an equivalent of 3.2 years of optimal health. Although not a formal cost-effectiveness analysis, this survey underscores the significant disease burden experienced by chronic migraine patients.
The health utility data on chronic migraine is sparse in the current literature, and there are even fewer papers that have reported prospective health utility results specifically on chronic migraine. Altura and colleagues used health utility indexes (HUI) to assess chronic migraine in the Canadian population. They found males had poorer HUI than females and were more likely to be limited in job and education opportunities14. Interestingly, our results found no statistically significant differences between men and women, with women actually having a slightly worse HUI across our three measures. However, the small sample size was not specifically powered to detect this potential difference. Additionally, HUI is a different measure of health status based on a health utility that only consists of eight attributes. These consist of vision, hearing, speech, ambulation, dexterity, emotion, cognition, and pain. This does not assess a patient’s desire for a resolution of their diagnosis, as the SG and TTO tests do. While there have been studies showing a disutility of 0.493 for severe acute migraine attacks, patients only met the criteria for episodic migraine and not chronic migraine. Additionally, the study was conducted 15 years ago, before most first-line treatments were available15. While there have been several studies assessing the economic burden of chronic migraine, these studies did not focus on assessing patient health utility. Still, these clinical trials assessed migraine treatment topiramate that provided Short Form Survey 36 (SF-36) at the time of enrollment16-18. These have been extrapolated through mapping to provide EQ-5D-5L data for manuscripts attempting to assess the QALY of an intervention, but are clinically limited because they were not specifically designed to assess health utility19. Our study has the advantage of directly assessing EQ-5D-5L, VAS, TTO, and SG for robust assessments of patients’ health utility.
Overall, the present study’s findings provide valuable insights into the health utility of patients with chronic migraine. Using the mean SG, TTO, and VAS scores, the study results clearly show that patients with chronic migraine have a lower quality of life compared to the general population. The QALY estimated from the TTO validated measure scores is 0.73, indicating a lower quality of life of patients with chronic migraine, even when adjusted for the average QALY of a person without chronic migraine but with other comorbidities. Therefore, healthcare providers and research funding should prioritize the management and advancement of the care and treatments for chronic migraine patients to improve the health utility and overall quality of life of patients.
Limitations and Future Studies
While health utility assessment is a valuable tool for evaluating the impact of different diagnoses on patients’ quality of life, our study does have limitations in that it was not powered to be a formal economic analysis study. Additionally, 25.6% of patients who were surveyed were excluded due to failing to submit survey results that gave monocular blindness an equal or worse disease burden compared to binocular blindness. Some patients may have genuinely perceived monocular blindness as worse than binocular blindness, submitting valid surveys. However, this conservative approach was adopted to ensure data reliability. When analyzed together with the excluded data, chronic migraine continued to show a worse disease burden compared to the other diseases, with more statistically significant differences. We want to emphasize that this is a descriptive paper. We did not power our survey to find statistical differences; rather, we are looking to provide health economic data quantifying the significance of impairment of quality of life for patients with chronic migraine. This study aims to help provide healthcare economists with directly assessed health utility scores to strengthen any formal QALY analysis regarding chronic migraine. Still, we did find that there are some differences across disease states and compared to the typical health utility score of those that highlight the significance of chronic migraine disease burden in a quantitative way. Furthermore, there is the potential age bias given that the survey was administered only in electronic format. Younger patients are more likely to be proficient with computer-based survey platforms. The patient population was predominantly Caucasian (82.8%) and would not represent the percentage demographics found throughout the United States, potentially presenting bias to our data and not allowing it to be extrapolated to other populations. Despite the limitations, this study highlights that chronic migraine patients perceive their disease burden causes a 20-30% worse quality of life compared to other chronic diseases, which is useful information about health utility scores for these patients for policymakers and economists. Further research is needed to understand the impact of migraines on patients’ quality of life in different contexts and patient populations. The challenge of finding comparable surveys to compare the results of this study with previous research in chronic migraine underscores the need to consider disease severity and patient context when interpreting health utility scores for not only this disease but others as well. Additionally, studies assessing the perceived health utility in chronic migraine patients would provide further insight into the impact new treatments would have. These studies have been conducted in other disease states, such as hair loss and rhinectomy defects20, 21, quantifying the significance of each disease state. Understanding the differences between experienced health utility for those with the diagnosis and perceived health utility by laypersons would further refine QALY cost modeling for healthcare economists.
Conclusion
To our knowledge, this study is the first to conduct a health utility study surveying patients with a chronic migraine diagnosis and present descriptive statistics demonstrating the severe negative impact of chronic migraine on health utility. Further large-scale, appropriately powered studies are needed to refine the quantification of the significance of this disease.
Tables
References
- Brown JS, Neumann PJ, Papadopoulos G, Ruoff G, Diamond M, Menzin J. Migraine frequency and health utilities: findings from a multisite survey. Value Health. Mar-Apr 2008;11(2):315-21. PubMed PMID: 18380644. doi:10.1111/j.1524-4733.2007.00246.x
- Burch R, Rizzoli P, Loder E. The prevalence and impact of migraine and severe headache in the United States: Updated age, sex, and socioeconomic-specific estimates from government health surveys. Headache. Jan 2021;61(1):60-68. PubMed PMID: 33349955. doi:10.1111/head.14024
- Ashina M, Buse DC, Ashina H, et al. Migraine: integrated approaches to clinical management and emerging treatments. Lancet. Apr 17 2021;397(10283):1505-1518. PubMed PMID: 33773612. doi:10.1016/S0140-6736(20)32342-4
- Lipton RB, Stewart WF, Diamond S, Diamond ML, Reed M. Prevalence and burden of migraine in the United States: data from the American Migraine Study II. Headache. Jul-Aug 2001;41(7):646-57. PubMed PMID: 11554952. doi:10.1046/j.1526-4610.2001.041007646.x
- Eltrafi A, Shrestha S, Ahmed A, Mistry H, Paudyal V, Khanal S. Economic burden of chronic migraine in OECD countries: a systematic review. Health Econ Rev. Sep 1 2023;13(1):43. PubMed PMID: 37656228; PubMed Central PMCID: PMCPMC10472624. doi:10.1186/s13561-023-00459-2
- Stang P, Cady R, Batenhorst A, Hoffman L. Workplace productivity. A review of the impact of migraine and its treatment. Pharmacoeconomics. 2001;19(3):231-44. PubMed PMID: 11303412. doi:10.2165/00019053-200119030-00002
- Headache Classification Committee of the International Headache S. The International Classification of Headache Disorders, 3rd edition (beta version). Cephalalgia. Jul 2013;33(9):629-808. PubMed PMID: 23771276. doi:10.1177/0333102413485658
- Harris PA, Taylor R, Thielke R, Payne J, Gonzalez N, Conde JG. Research electronic data capture (REDCap)–a metadata-driven methodology and workflow process for providing translational research informatics support. J Biomed Inform. Apr 2009;42(2):377-81. PubMed PMID: 18929686; PubMed Central PMCID: PMCPMC2700030. doi:10.1016/j.jbi.2008.08.010
- Harris PA, Taylor R, Minor BL, et al. The REDCap consortium: Building an international community of software platform partners. J Biomed Inform. Jul 2019;95:103208. PubMed PMID: 31078660; PubMed Central PMCID: PMCPMC7254481. doi:10.1016/j.jbi.2019.103208
- Drummond MF SM, Claxton K, Stoddart GL, Torrance GW. Methods for the Economic Evaluation of Health Care Programmes. 4th Edition ed. Oxford University Press; 2015.
- Pickard AS, Law EH, Jiang R, et al. United States Valuation of EQ-5D-5L Health States Using an International Protocol. Value Health. Aug 2019;22(8):931-941. PubMed PMID: 31426935. doi:10.1016/j.jval.2019.02.009
- Shaw JW, Johnson JA, Coons SJ. US valuation of the EQ-5D health states: development and testing of the D1 valuation model. Med Care. Mar 2005;43(3):203-20. PubMed PMID: 15725977. doi:10.1097/00005650-200503000-00003
- Xiao R, Burks CA, Yau J, et al. Health Utility Measures Among Patients with Androgenetic Alopecia After Hair Transplant. Aesthetic Plast Surg. Apr 2023;47(2):631-639. PubMed PMID: 35999465. doi:10.1007/s00266-022-03066-4
- Altura KC, Patten SB, Williams JVA, Fiest KM, Jette N. Living with Migraine in Canada – A National Community-Based Study. Can J Neurol Sci. Mar 2019;46(2):216-223. PubMed PMID: 30816083. doi:10.1017/cjn.2019.3
- Xu R, Insinga RP, Golden W, Hu XH. EuroQol (EQ-5D) health utility scores for patients with migraine. Qual Life Res. May 2011;20(4):601-8. PubMed PMID: 21063786. doi:10.1007/s11136-010-9783-5
- Brandes JL, Saper JR, Diamond M, et al. Topiramate for migraine prevention: a randomized controlled trial. JAMA. Feb 25 2004;291(8):965-73. PubMed PMID: 14982912. doi:10.1001/jama.291.8.965
- Diener HC, Tfelt-Hansen P, Dahlof C, et al. Topiramate in migraine prophylaxis–results from a placebo-controlled trial with propranolol as an active control. J Neurol. Aug 2004;251(8):943-50. PubMed PMID: 15316798. doi:10.1007/s00415-004-0464-6
- Silberstein SD, Neto W, Schmitt J, Jacobs D, Group M-S. Topiramate in migraine prevention: results of a large controlled trial. Arch Neurol. Apr 2004;61(4):490-5. PubMed PMID: 15096395. doi:10.1001/archneur.61.4.490
- Brown JS, Papadopoulos G, Neumann PJ, Friedman M, Miller JD, Menzin J. Cost-effectiveness of topiramate in migraine prevention: results from a pharmacoeconomic model of topiramate treatment. Headache. Sep 2005;45(8):1012-22. PubMed PMID: 16109115. doi:10.1111/j.1526-4610.2005.05182.x
- Abt NB, Quatela O, Heiser A, Jowett N, Tessler O, Lee LN. Association of Hair Loss With Health Utility Measurements Before and After Hair Transplant Surgery in Men and Women. JAMA Facial Plast Surg. Dec 1 2018;20(6):495-500. PubMed PMID: 30242313; PubMed Central PMCID: PMCPMC6248210. doi:10.1001/jamafacial.2018.1052
- Faris C, Heiser A, Quatela O, et al. Health utility of rhinectomy, surgical nasal reconstruction, and prosthetic rehabilitation. Laryngoscope. Jul 2020;130(7):1674-1679. PubMed PMID: 31846094. doi:10.1002/lary.28480
Declarations/Disclosures
Funding/Conflicts of interest: In compliance with the ICMJE uniform disclosure form, author declares the following:
Payment/services info: Author has declared that no financial support was received from any organization for the submitted work.
Financial relationships: Author have declared that they have no financial relationships at present or within the previous three years with any organizations that might have an interest in the submitted work.
Other relationships: Author have declared that there are no other relationships or activities that could appear to have influenced the submitted work.
Prior Presentation: Parts of this manuscript were presented before as an oral presentation at the 6th World Congress on Regional Anesthesia and Pain Medicine in Paris, France, where it won 2nd prize in the oral presentation chronic pain medicine category.