Author: Mark W Weatherall MB BC PhD FRCP FRCP Edin *1, Divyen Vanniasegaram MB BS BSc FHEA 2
Author Affiliation:
1 Department of Neurology, Stoke Mandeville Hospital, Mandeville Road, Aylesbury HP21 8AL, UK.
2 Croydon University Hospital, London Road, Thornton Health CR7 7YE, UK.
Competing Interests: The author/s declare no competing interests.
Issue: 17.02
DOI: 10.30756/ahmj.2026.17.02
Submitted: Mar 13, 2025
Revisions received: Mar 8, 2026
Accepted: Mar 16, 2026
Published: Mar 26, 2026
Recommended Citation: Weatherall MW, Vanniasegaram D. Greater Occipital Nerve Blockade: Safety, Adverse Effects, And Patient Outcomes In 1577 Injections. Ann Head Med. 2026;17:02. DOI: 10.30756/ahmj.2026.17.02
Background and objectives: Greater occipital nerve (GON) blockade is used to treat primary and secondary headache disorders. The primary objective of this study was to establish the safety and frequency of adverse events associated with GON blockade. Secondary objectives included recording patient-reported outcomes to provide real world data on the utility and consistency of the intervention. Material and methods: We performed a service evaluation of 1577 injections performed in 861 patients over a ten-year period. Results and conclusions: Immediate complications were recorded in 32 cases, the most common of which was near-syncope. Delayed effects were reported in 145 cases, mostly commonly persistent pain at the injection site. Serious side effects were rare. Follow-up data was available for 733/861 first injections. 36% of these patients reported an excellent or good response, 25% a fair or minimal response, 35% no response, and 4% were worse. The median duration of effect was two months. We conclude that GON blockade, even if repeated multiple times, is a safe and potentially useful intervention.
Introduction
Greater occipital nerve blockade is widely used as a treatment for primary and secondary headache disorders. The use of this intervention in the management of headache dates back to 1940,1 but came into widespread use after reports that it was a useful treatment for occipital neuralgia, 2 and subsequently for a number of primary headache disorders, including migraine,2, 3 menstrual migraine,4 cluster headache,5-8 chronic cluster headache,9-11 and hemicrania continua,3 as well as cervicogenic headache,12, 13 coital cephalalgia,14 and trigeminal neuropathy.15 Recent placebo-controlled trials – in migraine, chronic migraine, and medication overuse headache – are less consistent, though meta-analysis suggests a probable overall benefit. 16-22
We performed a service evaluation of 1577 injections performed in 861 patients over a ten-year period. The primary objective was to establish the safety and frequency of adverse events in a large cohort of patients, including a significant number who underwent repeated injections. Secondary objectives included recording patient-reported outcomes to provide real world data on the utility and consistency of the intervention.
Methods
Patients were seen in a general neurology clinic at a district general hospital in West London, a specialized adult headache clinic embedded within a regional neurosciences center, and in private practice, between 2007-2017. Information was collected as part of the standard history-taking in a normal consultation. A retrospective review of medical records was undertaken by the authors. Information was recorded on the age and sex of the patient, the main headache diagnosis, the location and quantity of materials injected, immediate complications, and if available, subsequent adverse events and patient-reported outcome (frequency and severity of headaches). Data collection for this study comprises a retrospective chart review, and as such, did not require specific consent, as confirmed by the Joint Research Compliance Office at Imperial College.
Headache diagnoses were made according to the then current version of the International Classification of Headache Disorders (ICHD-2 prior to 2013; ICHD-3 beta thereafter). Where patients had more than headache diagnosis, only the most clinically significant diagnosis was recorded for this analysis. The diagnosis of cervicogenic headache (ICHD-3 11.2.1) was made in patients in whom their typical (and most troublesome) headache was provoked either by palpation of neck structures, or by head movement, or both. Patients were considered for treatment with greater occipital nerve blockade if they had pain arising from the nerve/s or related neck structures, had a lateralized primary headache diagnosis accompanied with ipsilateral occipital nerve tenderness, or had a global headache associated with bilateral occipital nerve tenderness. Patients received methylprednisolone 80 mg (+/- 40 mg) and 2 mL 2% lidocaine. A landmark approach was used, locating the greater occipital nerve one-third of the way between the occipital protuberance and the mastoid process. Injections were given at the most tender point/s on palpation over the course of the nerve, using a 25 g or 27 g needle, inserted at 45º in a rostral direction down to the periosteum, before withdrawing slightly, and pulling back on the needle to ensure that the solution was not injected into a vascular structure.
Patient outcomes were stratified as follows: Excellent: decreased frequency and severity of headaches for ≥3 months; Good: decreased frequency and severity of headaches for 1-3 months, or decreased frequency or severity for ≥3 months; Fair: decreased frequency and severity of headaches for 1-4 weeks, or decreased frequency or severity for 1-3 months; Minimal: decreased frequency and severity for <1 week, or decreased frequency or severity for <1 month; None: no effect; Worse: worsening of headaches for >1 week.
Results
Records of 1577 injections performed in 861 patients (662 F, 199 M) were identified. The mean age of patients was 46 (range 16-96). 546 patients had only a single injection. 169 patients had two injections, 66 had three, and 34 had four. 21 patients had ≥7 injections; three of those patients had 20, 21, and 23 injections, respectively.
The commonest primary diagnosis was chronic migraine (299/861), reflecting the high number of patients who were being seen in a tertiary referral headache service. There were also large numbers of patients with episodic migraine without aura (235), and neck-related head pain (cervicogenic headache 159, occipital neuralgia/entrapment neuropathy 65). There were 34 patients with chronic cluster headache, 15 with episodic cluster headache, 19 with episodic migraine with aura, and small numbers with other primary headache disorders such as chronic paroxysmal hemicrania, hemicrania continua, SUNA/SUNCT, and hypnic headache, as well as secondary disorders such as trigeminal and posterior auricular neuropathies.
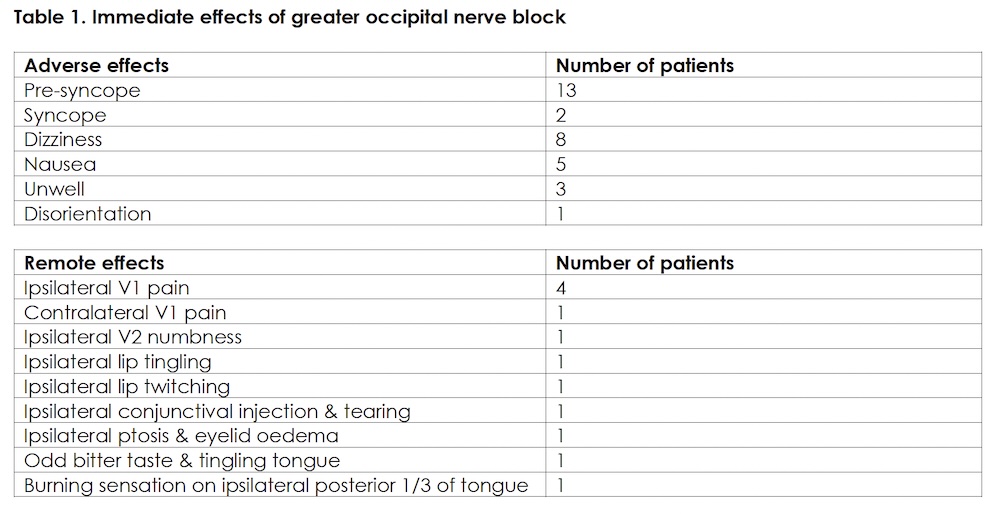
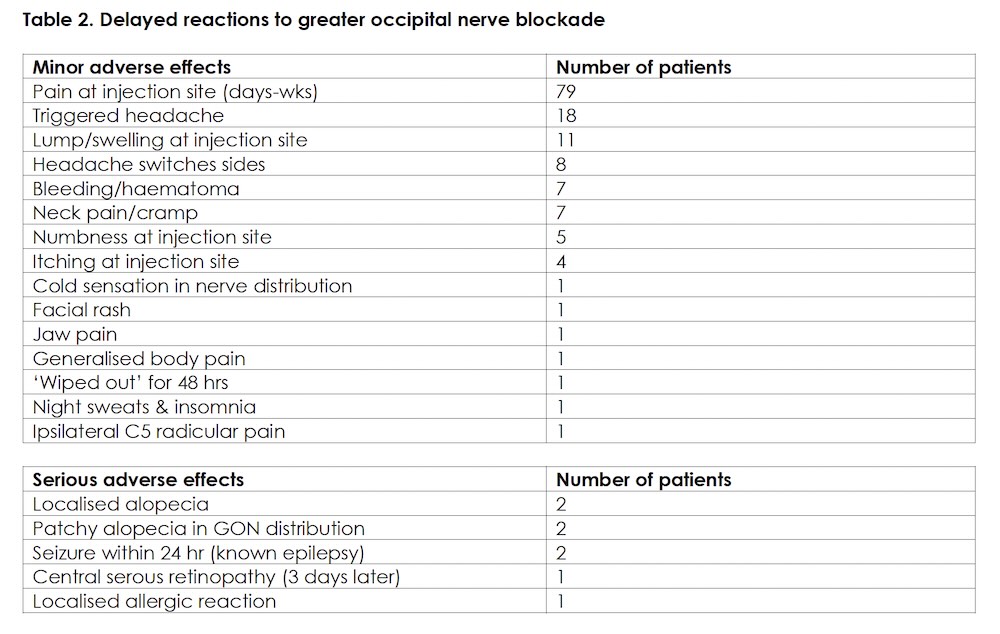
Immediate complications were recorded in 32/1577 cases, most commonly syncope or near-syncope. 12 patients reported immediate symptoms in ipsilateral or contralateral trigeminal territory or tongue, presumably mediated through activation of the trigeminocervical complex, or from stimulation of hypoglossal fibres in the ansa cervicalis. [Table 1] Delayed effects were reported in 145/1380 cases for which follow-up information was available. The most common adverse effect was persistent pain at the injection site. Serious side effects were rare: four cases of alopecia were recorded (two localized to the injection point, and two more patchily through the area supplied by the GON injected), two patients with known active epilepsy had seizures within 24 hours of the injection, one patient had a significant localized allergic reaction, and there was one case of central serous retinopathy closely temporally related to the injection. Given the proximity of vascular structures to the occipital nerve, it is noteworthy that there were very few vascular complications. [Table 2] 20 injections were given to women whilst pregnant, and 30 whilst breast-feeding, with no significant adverse consequences. 21 patients had ≥7 injections; two of the cases of alopecia occurred in this group but there was otherwise no evidence of any cumulative risk of adverse events from repeated injections.
Follow-up data was available for 733/861 first injections. 261 patients (36%) reported an excellent or good response, 184 (25%) a fair or minimal response, 256 (35%) no response, and 32 (4%) were worse. For those who responded (445 patients), the median duration of effect was two months; 149 (34%) derived <4 weeks’ benefit; 236 (53%) derived between 5-12 weeks’ benefit; and 60 (13%) derived >3 months’ benefit. For episodic migraine without aura (235 patients), the outcomes were virtually identical to the population as a whole (37% excellent or good; 24% fair or minimal; 33% no effect; 6% worse); for chronic migraine the outcomes were less positive (26% excellent or good; 27% fair or minimal; 41% no effect; 6% worse); and for neck-related headaches, somewhat more positive (51% excellent or good; 20% fair or minimal; 27% no effect; 2% worse). Numbers were small in the other headache phenotypes, but there were no obvious significant divergences from the outcome figures for the population as a whole.
Of those patients for whom ongoing follow-up was available, 24/34 (71%) patients who did not respond to a first injection failed to respond to a second injection or got worse. Conversely, 70/119 (59%) of those who reported a good response to the first injection, did as well or better with a second injection, although 32 of these patients (27%) did not respond to the second injection.
Discussion
GON blockade is now widely used in specialist headache centers around the world. This study confirms the findings of previously published case series of GON blockade, in that it is seen to be a safe and useful treatment for patients with primary and secondary headache disorders. Real world evidence has significant limitations, as outcome data is highly prone to multiple forms of bias. Nonetheless data of the type presented in this paper is helpful in answering some questions relevant to patient management, specifically whether the safety and adverse event data presented in previous smaller series remain applicable in cases where patients receive multiple injections over time (it does); whether patients who respond to GON blocks are likely to respond again to future blocks (they are); and whether it is worth trying the intervention again if it does not work first time (it is probably not). It is also clear that the simple office-based technique used in this study is not associated with significant risks of damage to adjacent vascular structures, thus reducing the necessity of performing occipital nerve blockade under ultrasound guidance, which may have implications for accessibility and cost of the intervention. Whether the more precise blockade that can be achieved under ultrasound guidance improves outcomes overall remains a matter of debate.23
The question remains: what are we treating with greater occipital nerve blockade? Since the early 1990s many studies have shown that targeting peripheral nervous system inputs into the trigeminocervical complex can be a viable option for treating intractable headache disorders. The pathophysiological basis for the responses to blockade of the GON in patients with primary headache disorders is believed to relate to the modulation of input into neuronal processing in the trigeminocervical complex (TCC),24, 25 where second order neurons have input from both trigeminal and cervical afferents. The fibres of the GON originate predominantly from the C2 dorsal root, and stimulation of the nerve activates neurons in the TCC; in some cases this can elicit ipsilateral conjunctival injection, eye watering, and ptosis.26 Stimulation of the C1 and C2 nerve roots can elicit frontal pain, especially in patients with migraine.27 Even transient alterations to the input from the greater occipital nerve may therefore precipitate a central modulatory changes involving the TCC, providing an explanation for the effect of GON blockade in primary headache disorders. One study suggests that GON blockade may reduce interictal serum CGRP levels, which are generally elevated in chronic migraine.28 In other cases it is clear that there is entrapment of the nerve or nerves as they pass through the suboccipital muscle layers. Peripheral nerve entrapment of this nature can itself cause pain in the distribution of the nerve; herein lies the explanation for the efficacy of GON blockade in neck-related secondary headache disorders.
It is noteworthy that the overall response rates to initial GON blockade were very similar for all the main primary headache phenotypes represented in this study, with only a very slight trend towards a less positive response in chronic migraine. The rather better response seen in neck-related headaches may indicate that in some cases, the pathology lies at the site of the injection itself, specifically relating to occipital nerve entrapment. In cases where patients derive consistent but transient benefit, referral for occipital nerve decompression may be indicated, whatever the main headache diagnosis.29, 30
Conclusion
In conclusion, the clinical implications of this study are that GON blockade is a safe intervention for patients with primary and secondary headache disorders; serious adverse events are very rare and, with the possible exception of alopecia, repeated injections are not associated with higher risks of adverse effects; more than 50% of patients will derive some benefit from the intervention; and the response to the first injection is a good guide to likely response to further injections.
Tables
References
- Hadden S. Neuralgic headache and facial pain. Arch Neurol Psychiatry. 1940;43:405–08.
- Anthony M. Headache and the greater occipital nerve. Clin Neurol Neurosurg. 1992;94(4):297-301. PubMed PMID: 1335856. doi:10.1016/0303-8467(92)90177-5
- Afridi SK, Shields KG, Bhola R, Goadsby PJ. Greater occipital nerve injection in primary headache syndromes–prolonged effects from a single injection. Pain. May 2006;122(1-2):126-9. PubMed PMID: 16527404. doi:10.1016/j.pain.2006.01.016
- Cetin G, Totuk O, Cetin OE, Demir S, Sahin S. Evaluation of the effectiveness of greater occipital nerve blockade in menstrual migraine. BMC Neurol. Feb 13 2025;25(1):62. PubMed PMID: 39948478; PubMed Central PMCID: PMCPMC11823226. doi:10.1186/s12883-025-04070-2
- Peres MF, Stiles MA, Siow HC, Rozen TD, Young WB, Silberstein SD. Greater occipital nerve blockade for cluster headache. Cephalalgia. Sep 2002;22(7):520-2. PubMed PMID: 12230593. doi:10.1046/j.1468-2982.2002.00410.x
- Ambrosini A VM, Rossi P, et al. Suboccipital (GON) injection with long acting steroids in cluster headache: a double-blind placebo-controlled study. . Cephalalgia. 2003;23:734.
- Chowdhury D, Kordcal SR, Nagane R, Duggal A. ANODYNE study: A double-blind randomized trial of greater occipital nerve block of methylprednisolone and lignocaine versus placebo as a transitional preventive treatment for episodic cluster headache. Cephalalgia. Oct 2024;44(10):3331024241291597. PubMed PMID: 39415681. doi:10.1177/03331024241291597
- Gordon A, Roe T, Villar-Martinez MD, Moreno-Ajona D, Goadsby PJ, Hoffmann J. Effectiveness and safety profile of greater occipital nerve blockade in cluster headache: a systematic review. J Neurol Neurosurg Psychiatry. Dec 14 2023;95(1):73-85. PubMed PMID: 36948579. doi:10.1136/jnnp-2023-331066
- Gaul C, Roguski J, Dresler T, et al. Efficacy and safety of a single occipital nerve blockade in episodic and chronic cluster headache: A prospective observational study. Cephalalgia. Aug 2017;37(9):873-880. PubMed PMID: 27313215. doi:10.1177/0333102416654886
- Lambru G, Abu Bakar N, Stahlhut L, et al. Greater occipital nerve blocks in chronic cluster headache: a prospective open-label study. Eur J Neurol. Feb 2014;21(2):338-43. PubMed PMID: 24313966. doi:10.1111/ene.12321
- Karacan Golen M, Tepe N, Isik SM. Effectiveness of greater occipital nerve blockade in chronic cluster headache. Eur Rev Med Pharmacol Sci. Aug 2024;28(16):4170-4178. PubMed PMID: 39229846. doi:10.26355/eurrev_202408_36669
- Anthony M. Cervicogenic headache: prevalence and response to local steroid therapy. Clin Exp Rheumatol. Mar-Apr 2000;18(2 Suppl 19):S59-64. PubMed PMID: 10824289.
- Caponnetto V, Ornello R, Frattale I, et al. Efficacy and safety of greater occipital nerve block for the treatment of cervicogenic headache: a systematic review. Expert Rev Neurother. May 2021;21(5):591-597. PubMed PMID: 33709864. doi:10.1080/14737175.2021.1903320
- Selekler M, Kutlu A, Dundar G. Orgasmic headache responsive to greater occipital nerve blockade. Headache. Jan 2009;49(1):130-1. PubMed PMID: 18834455. doi:10.1111/j.1526-4610.2008.01253.x
- Weatherall MW. Idiopathic trigeminal neuropathy may respond to greater occipital nerve injection. Cephalalgia. Jun 2008;28(6):664-6. PubMed PMID: 18384417. doi:10.1111/j.1468-2982.2008.01561.x
- Dilli E, Halker R, Vargas B, et al. Occipital nerve block for the short-term preventive treatment of migraine: A randomized, double-blinded, placebo-controlled study. Cephalalgia. Oct 2015;35(11):959-68. PubMed PMID: 25505035. doi:10.1177/0333102414561872
- Inan LE, Inan N, Karadas O, et al. Greater occipital nerve blockade for the treatment of chronic migraine: a randomized, multicenter, double-blind, and placebo-controlled study. Acta Neurol Scand. Oct 2015;132(4):270-7. PubMed PMID: 25765043. doi:10.1111/ane.12393
- Gul HL, Ozon AO, Karadas O, Koc G, Inan LE. The efficacy of greater occipital nerve blockade in chronic migraine: A placebo-controlled study. Acta Neurol Scand. Aug 2017;136(2):138-144. PubMed PMID: 27910088. doi:10.1111/ane.12716
- Karadas O, Ozon AO, Ozcelik F, Ozge A. Greater occipital nerve block in the treatment of triptan-overuse headache: A randomized comparative study. Acta Neurol Scand. Apr 2017;135(4):426-433. PubMed PMID: 27666722. doi:10.1111/ane.12692
- Cuadrado ML, Aledo-Serrano A, Navarro P, et al. Short-term effects of greater occipital nerve blocks in chronic migraine: A double-blind, randomised, placebo-controlled clinical trial. Cephalalgia. Aug 2017;37(9):864-872. PubMed PMID: 27296456. doi:10.1177/0333102416655159
- Zhang H, Yang X, Lin Y, Chen L, Ye H. The efficacy of greater occipital nerve block for the treatment of migraine: A systematic review and meta-analysis. Clin Neurol Neurosurg. Feb 2018;165:129-133. PubMed PMID: 29421172. doi:10.1016/j.clineuro.2017.12.026
- Chowdhury D, Tomar A, Deorari V, Duggal A, Krishnan A, Koul A. Greater occipital nerve blockade for the preventive treatment of chronic migraine: A randomized double-blind placebo-controlled study. Cephalalgia. Feb 2023;43(2):3331024221143541. PubMed PMID: 36739512. doi:10.1177/03331024221143541
- Gursoy G, Tuna HA. Comparison of two methods of greater occipital nerve block in patients with chronic migraine: ultrasound-guided and landmark-based techniques. BMC Neurol. Sep 4 2024;24(1):311. PubMed PMID: 39232647; PubMed Central PMCID: PMCPMC11373286. doi:10.1186/s12883-024-03816-8
- Bartsch TaG, P.J. Anatomy and Physiology of Pain Referral Patterns in Primary and Cervicogenic Headache Disorders. Headache Currents. 2005;2:42-48. doi:10.1111/j.1743-5013.2005.20201.x
- Busch V, Jakob W, Juergens T, Schulte-Mattler W, Kaube H, May A. Functional connectivity between trigeminal and occipital nerves revealed by occipital nerve blockade and nociceptive blink reflexes. Cephalalgia. Jan 2006;26(1):50-5. PubMed PMID: 16396666. doi:10.1111/j.1468-2982.2005.00992.x
- Goadsby PJ, Knight YE, Hoskin KL. Stimulation of the greater occipital nerve increases metabolic activity in the trigeminal nucleus caudalis and cervical dorsal horn of the cat. Pain. Oct 1997;73(1):23-8. PubMed PMID: 9414053. doi:10.1016/s0304-3959(97)00074-2
- Johnston MM, Jordan SE, Charles AC. Pain referral patterns of the C1 to C3 nerves: implications for headache disorders. Ann Neurol. Jul 2013;74(1):145-8. PubMed PMID: 23424170. doi:10.1002/ana.23869
- Abbas A, Moustafa R, Shalash A, et al. Serum CGRP Changes following Ultrasound-Guided Bilateral Greater-Occipital-Nerve Block. Neurol Int. Feb 7 2022;14(1):199-206. PubMed PMID: 35225886; PubMed Central PMCID: PMCPMC8883968. doi:10.3390/neurolint14010016
- Blake P, Nir RR, Perry CJ, Burstein R. Tracking patients with chronic occipital headache after occipital nerve decompression surgery: A case series. Cephalalgia. Apr 2019;39(4):556-563. PubMed PMID: 30217120; PubMed Central PMCID: PMCPMC7164296. doi:10.1177/0333102418801585
- Eskilsson A, Ageberg E, Ericson H, Marklund N, Anderberg L. Decompression of the greater occipital nerve improves outcome in patients with chronic headache and neck pain – a retrospective cohort study. Acta Neurochir (Wien). Sep 2021;163(9):2425-2433. PubMed PMID: 34195861; PubMed Central PMCID: PMCPMC8357752. doi:10.1007/s00701-021-04913-0
Declarations/Disclosures
Funding/Conflicts of interest: In compliance with the ICMJE uniform disclosure form, authors declares the following:
Payment/services info: Authors have declared that no financial support was received from any organization for the submitted work.
Financial relationships: Authors have declared that they have no financial relationships at present or within the previous three years with any organizations that might have an interest in the submitted work.
Other relationships: Authors have declared that there are no other relationships or activities that could appear to have influenced the submitted work.