Author: Roy Sebastian MD, DPT, MBA*1, Eleanor Seo MS4 2, Sweta Sengupta MD 3
Author Affiliation:
1 Dept. of Anesthesiology (Pain medicine), University of Maryland Medical Center, Baltimore, MD.
2 Duke University School of Medicine, Durham, NC.
3 Dept. of Neurology- Headache Medicine, Duke University Medical Center, Durham, NC.
Competing Interests: The author/s declare no competing interests.
Issue: 16.01
DOI: 10.30756/ahmj.2025.16.01
Received: Sept 11, 2025
Accepted: Nov 12, 2025
Published: Nov 26, 2025
Recommended Citation: Sebastian R, Seo E, Sengupta S. Cervical Osteomyelitis With Epidural Abscess Overlooked In A Patient With Migraine And Idiopathic Intracranial Hypertension: A Case Report. Ann Head Med. 2025;16:01. DOI: 10.30756/ahmj.2025.16.01
In patients with migraine or idiopathic intracranial hypertension (IIH) a worsening headache can often be attributed to an increase in intracranial pressure. Associated symptoms like new onset or worsening neck pain may be masked by this diagnosis, delaying identification of other serious conditions like cervical osteomyelitis. We present a female in her thirties with a medical history of episodic migraine, idiopathic intracranial hypertension without papilledema (IIHWOP), and type two diabetes mellitus, who developed worsening headaches with neck pain, photophobia, vertigo, and weight loss. Standard migraine therapies were ineffective. Neurological exams, fundoscopy, brain and vascular imaging, and lumbar puncture were unremarkable. A cervical spine MRI revealed findings consistent with cervical osteomyelitis and an epidural abscess. Cultures confirmed methicillin-resistant Staphylococcus aureus (MRSA). She was treated with antibiotics and monitored by infectious disease and neurology. Follow-up imaging showed improvement, and she continued conservative treatment with close specialist follow-up. This case underscores the importance of maintaining a broad differential diagnosis in patients with worsening headache features, particularly when associated with red flag symptoms such as neck pain and systemic signs, to avoid delays in diagnosing potentially life-threatening conditions such as spinal infections.
Background
In patients with pre-existing medical conditions such as episodic migraine or idiopathic intracranial hypertension without papilledema (IIHWOP), new or worsening headache is typically attributed to intracranial pressure changes. Such a presumption can delay consideration of differential diagnoses when other symptoms such as neck pain, photophobia, or systemic symptoms are subtle or nonspecific. In these cases, secondary or related pathology- such as spinal infection-may be overlooked when initial neurologic studies and laboratory test results are unremarkable.
Cervical osteomyelitis and epidural abscesses secondary to it are uncommon but serious diseases that can present as headache, neck pain, and constitutional symptoms. Early diagnosis is of greatest importance but can be challenging, particularly in patients with long-standing headache disorders and comorbid diseases such as diabetes mellitus. Diagnostic evaluation can also be rendered more difficult by recent treatment. For instance, leukocytosis is expected in patients on corticosteroids which may mask underlying infection especially in patients without systemic symptoms. On the contrary, inflammatory markers such as C-reactive protein (CRP) and erythrocyte sedimentation rate (ESR) are more likely to provide better evaluation of systemic inflammation in this context but are not routinely ordered.
This case presents the diagnostic dilemma of a patient with history of migraine and IIHWOP with recurrent headache, neck pain, and systemic symptoms and ultimately diagnosed with cervical osteomyelitis and an epidural abscess secondary to methicillin-resistant Staphylococcus aureus (MRSA).
Case presentation
A woman in her thirties with a medical history of episodic migraine, idiopathic intracranial hypertension without papilledema (IIHWOP), type 2 diabetes mellitus, hypothyroidism, and obesity presented to the headache clinic for evaluation of progressively worsening headaches. Two months prior, she had been hospitalized for bilateral pneumonia and lower extremity cellulitis, for which she was treated with doxycycline and subsequently discharged. A month later, she underwent a left adrenalectomy for a cortisol-secreting adrenal adenoma and started on hydrocortisone replacement therapy.
Throughout the postoperative course, her episodic migraines suddenly transitioned to daily, burning headaches that were accompanied by photophobia, vertigo, pulsatile tinnitus, and brief visual blurring. She was evaluated multiple times at the emergency department (ED), where neurological examination and brain imaging [Computed Tomography (CT) and Magnetic Resonance Imaging (MRI)] were normal. She was empirically started on topiramate for presumed vestibular migraine and increased dose of acetazolamide for presumed worsening of IIH. There was initial relief with an occipital nerve block, but she rapidly relapsed and her symptoms continued to worsen. Notably, repeated leukocytosis was observed on several occasions but were assumed to be secondary to her recent corticosteroids, and inflammatory markers such as CRP and ESR were not initially quantified.
On a return visit to the headache clinic after her third visit to the ED, she presented with severe positional headaches and posterior neck pain that had recently begun. Worsening with head movement and partially relieved by sleeping in a position with raised head was her presentation. Her mother also reported that tender head and neck massage relieved the symptoms every time, information that raised clinical suspicion of cervical involvement. Neurologic exam was largely benign other than for residual sensory deficits in the left V2-V3 trigeminal dermatomes. There were no new medications initiated at the time, but due to the residual symptoms and the unusual pain relief pattern, MRI of the cervical spine was ordered.
Prior to the scheduled MRI of the cervical spine, the patient returned to the ED with worsening symptoms. She was given a migraine cocktail and discharged on sumatriptan. With recurrent symptoms, she was admitted for dihydroergotamine (DHE) infusions for intractable migraine and accompanying visual changes. Her neurological exam and bedside fundoscopy were within normal limits, but lumbar puncture showed an opening pressure of 31 cm H₂O, which is compatible with mildly elevated intracranial pressure.
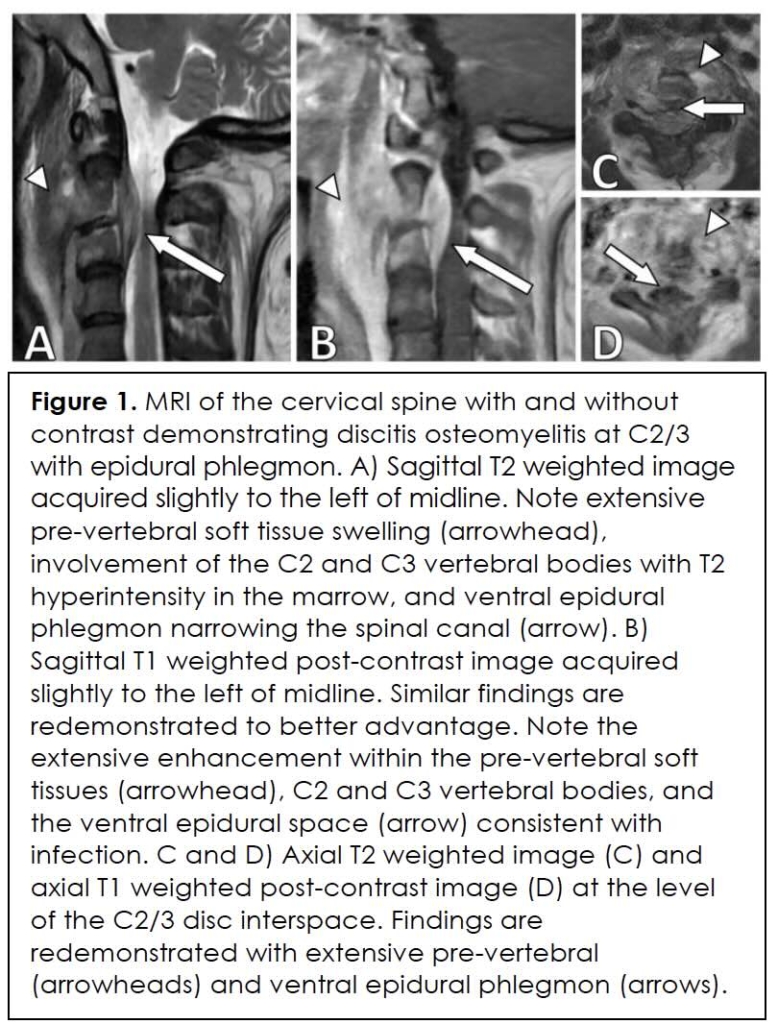
In view of continued deterioration of neck pain and headache, the earlier scheduled cervical spine MRI was performed soon after the ED visit. Imaging revealed abnormal enhancement and edema at C2-C3 vertebral levels with accompanying narrowing of the spinal canal consistent with osteomyelitis and an epidural abscess (Figure 1). Biopsy under CT guidance was confirmed, with cultures showing methicillin-resistant Staphylococcus aureus (MRSA). During this period, inflammatory markers were significantly elevated: white blood cell count 11.2 × 10⁹/L, CRP 7.35 mg/dL, and ESR 114 mm/hr. Thoracic spine MRI revealed additional foci of vertebral osteomyelitis.
The patient was started on intravenous vancomycin and ceftriaxone and was discharged on a peripherally inserted central catheter (PICC) line for six weeks’ intravenous antibiotics as an outpatient. She was followed closely by infectious disease and neurology services. On follow-up, she improved over time, and follow-up imaging showed resolution of the cervical abscess.
This case illustrates the diagnostic challenge of diagnosing cervical osteomyelitis in patients with overlapping headache syndromes. It also underscores the importance of maintaining a broad differential diagnosis in patients with evolving symptoms, particularly in those with risk factors for infection such as surgery, diabetes, and immunosuppression.
Investigations
Initial investigations focused on ruling out emergent causes of headache, including acute intracranial hemorrhage and venous sinus thrombosis, using MRI of the brain with and without contrast and a CT venogram of the head. Evaluation for increased intracranial pressure included slit-lamp fundoscopic examination and lumbar puncture, which revealed a mildly elevated opening pressure. As her symptoms progressed, particularly with focal neck pain, an MRI of the cervical spine was performed, revealing lesions at the C2-C3 vertebrae. A biopsy and culture confirmed cervical osteomyelitis and an epidural abscess due to methicillin-resistant Staphylococcusaureus (MRSA). Inflammatory markers were not obtained when she first presented but were significantly elevated when the infectious etiology was suspected. Finally, further thoracic MRI revealed no additional lesions.
Differential Diagnosis
The differential diagnosis in a patient with episodic migraines is extensive when presents with daily severe headaches with a positional component, neck pain and dizziness. It includes conditions related to venous drainage such as cerebral venous sinus thrombosis and dural arteriovenous fistulas; central nervous system infections such as meningitis; mass lesions secondary to prior hemorrhage, neoplastic process, or paraspinal abscesses; drug side effects; and endocrinopathies, such as adrenal insufficiency 1-7.
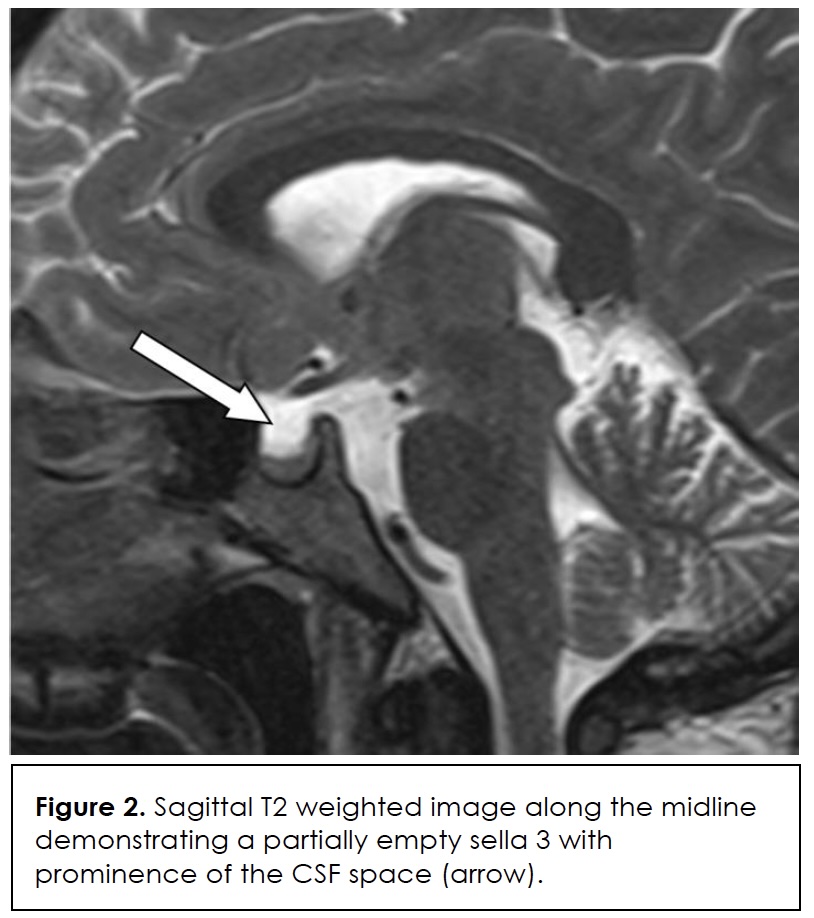
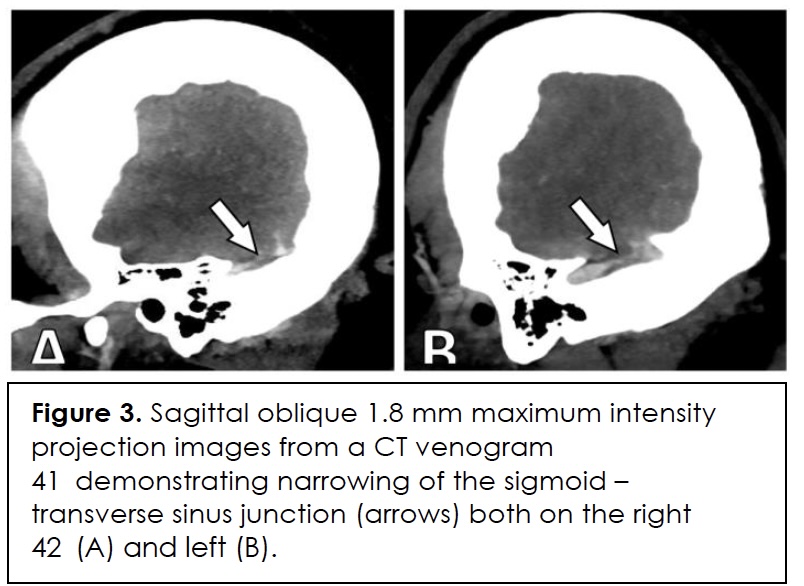
In this case, diagnostic specificity was also undermined by the patient’s simultaneous risk factors for infection and immunosuppression such as type 2 diabetes, obesity, recent adrenalectomy, and corticosteroid therapy. Her migraine history and probable idiopathic intracranial hypertension without papilledema (IIHWOP) initially predisposed towards a primary headache diagnosis. Brain imaging ruled out an intracranial mass, and she met two radiographic criteria for IIHWOP – empty sella (Figure 2) and transverse sinus narrowing (Figure 3) – that are consistent with the modified Friedman criteria for diagnosis 8. However, inability to demonstrate papilledema and absence of a persistent response to therapy prompted further investigation.
Notably, her corticosteroids would have blunted normal inflammatory responses, obscuring the significance of her leukocytosis and submerging awareness of an underlying greater process. Only following cervical spine MRI, for persistent neck pain and atypical symptom relief from massage, was cervical osteomyelitis with an epidural abscess diagnosed.
This case points out the diagnostic challenge of distinguishing secondary causes of headache in comorbid patients with primary headache disorders, particularly if there is immunosuppression or other systemic risk factors.
This case underscores the diagnostic challenges of distinguishing secondary causes of headache in patients with overlapping primary headache disorders, particularly when immunosuppression or other systemic risk factors are present.
Treatment
The patient’s initial treatment focused on managing presumed migraine and idiopathic intracranial hypertension (IIH). She was started on topiramate, followed by an occipital nerve block during a subsequent ED visit for localized tenderness. Due to side effects, topiramate was discontinued and replaced with acetazolamide, quetiapine, and a prednisone taper. Despite temporary relief, her headaches persisted, and sumatriptan was added. As symptoms continued, her regimen was adjusted to include indomethacin, propranolol, and a higher dose of sumatriptan. She was later hospitalized for intractable headache and received intravenous dihydroergotamine (DHE), which offered transient relief. After cervical spine imaging revealed osteomyelitis and an epidural abscess, she was treated with IV vancomycin, transitioned to daptomycin, and later doxycycline. Surgical intervention was considered but deferred as follow-up imaging showed abscess reduction.
Outcome And Follow-Up
The patient was discharged from the hospital with a peripherally inserted central catheter (PICC line) for a six-week course of antibiotics, and she was followed closely by infectious disease and neurology in an outpatient setting. One month after discharge, follow-up MRI reported unchanged osteomyelitis but decreased size of the epidural abscess. Two months later, she reported headache that, although decreased in frequency compared to initial presentation, was associated with new monocular diplopia. MRI brain showed no infectious changes, and she was referred to ophthalmology and was reassured that there was no papilledema. She continued to see outpatient neurology and be treated for chronic migraine with IIH.
Discussion
Our patient, with a known history of episodic migraine and IIHWOP, initially appeared to have an exacerbation of these primary conditions. She met two criteria for IIHWOP [8] but her persistent and progressively worsening symptoms did not fully align with her established diagnoses. The presence of left V1-V2 sensory deficits was initially attributed to migraine aura.
The delay in diagnosing cervical osteomyelitis and epidural abscess was partly due to the nonspecific nature of her early clinical and laboratory findings. Although CBC was routinely ordered, her WBC counts were largely within normal limits—consistent with literature indicating normal WBC in up to 40% of vertebral osteomyelitis cases 9, 10. ESR and CRP, which have higher sensitivity 11, were not initially measured during her ED visits. When they were eventually tested during hospitalization, both were markedly elevated, supporting an infectious etiology. In immunocompromised patients, including those on chronic steroids or with diabetes mellitus- as in this case- laboratory markers of infection may be falsely negative 12, 13. This further highlights the need for a high index of suspicion and timely use of advanced imaging and cultures for investigating possible vertebral osteomyelitis 14, which ultimately confirmed the diagnosis.
Patients with diabetes and adrenal insufficiency are at increased risk for spinal infections due to impaired immune responses, vascular insufficiency, and frequent exposure to healthcare settings 11, 15. In such populations, symptoms may be subtle and mimic other conditions, as seen here with headache and neck pain resembling chronic migraine or IIH. MRI remains the gold standard for diagnosing spinal infections and should be considered early when symptoms deviate from baseline or fail to respond to standard therapies 14. Ultimately, this case illustrates the need for comprehensive evaluation in patients with overlapping neurological and systemic conditions, particularly when they are immunosuppressed or have risk factors for infection. Additionally, given her continuing head pain, this case raises the possibility that cervical osteomyelitis and IIHWOP may have coexisted, both contributing to the patient’s clinical presentation.
This is further emphasized by similar cases of vertebral osteomyelitis being masked by the common complaint of back pain; in one, a historic compression fracture with suspected UTI delayed diagnosis 16, while in another, prompt lumbar spine imaging in a diabetic patient on empagliflozin quickly identified how asymptomatic bacteriuria led to vertebral osteomyelitis and iliopsoas abscess 17.
Learning Points
- Prior immunocompromised status or immunosuppressant medication use may mask infectious causes of headache via falsely reassuring CBC, ESR, and CRP.
- A CRP and ESR may still be beneficial in migraine patients with atypical symptoms or worsening conditions.
- Consider cervical spine imaging in patients with intractable headaches refractory to treatment, along with focal head and neck pain to palpation.
References
- Mollan SP, Ali F, Hassan-Smith G, Botfield H, Friedman DI, Sinclair AJ. Evolving evidence in adult idiopathic intracranial hypertension: pathophysiology and management. J Neurol Neurosurg Psychiatry. Sep 2016;87(9):982-92. PubMed PMID: 26888960; PubMed Central PMCID: PMCPMC5013119. doi:10.1136/jnnp-2015-311302
- Sadoghi M, Dabirmoghaddam P. Otitic hydrocephalus: case report and literature review. Am J Otolaryngol. May-Jun 2007;28(3):187-90. PubMed PMID: 17499137. doi:10.1016/j.amjoto.2006.07.007
- Van Dop C, Conte FA, Koch TK, Clark SJ, Wilson-Davis SL, Grumbach MM. Pseudotumor cerebri associated with initiation of levothyroxine therapy for juvenile hypothyroidism. N Engl J Med. May 5 1983;308(18):1076-80. PubMed PMID: 6835321. doi:10.1056/NEJM198305053081807
- Esmaili N, Bradfield YS. Pseudotumor cerebri in children with Down syndrome. Ophthalmology. Sep 2007;114(9):1773-8. PubMed PMID: 17368546. doi:10.1016/j.ophtha.2006.12.015
- Kalmar CL, Zapatero ZD, Kosyk MS, et al. Elevated intracranial pressure with craniosynostosis: a multivariate model of age, syndromic status, and number of involved cranial sutures. J Neurosurg Pediatr. Dec 1 2021;28(6):716-723. PubMed PMID: 34560658. doi:10.3171/2021.6.PEDS21162
- Adelman JU. Headaches and papilledema secondary to dural arteriovenous malformation. Headache. Sep 1998;38(8):621-3. PubMed PMID: 11398307. doi:10.1046/j.1526-4610.1998.3808621.x
- Pulhorn H, Chandran A, Nahser H, Wilby MJ, McMahon C. Intracranial Hypertension Secondary to Cervical Dural Arteriovenous Fistula. Asian J Neurosurg. Jul-Sep 2018;13(3):854-857. PubMed PMID: 30283565; PubMed Central PMCID: PMCPMC6159076. doi:10.4103/ajns.AJNS_328_16
- Friedman DI, Jacobson DM. Diagnostic criteria for idiopathic intracranial hypertension. Neurology. Nov 26 2002;59(10):1492-5. PubMed PMID: 12455560. doi:10.1212/01.wnl.0000029570.69134.1b
- Zimmerli W. Clinical practice. Vertebral osteomyelitis. N Engl J Med. Mar 18 2010;362(11):1022-9. PubMed PMID: 20237348. doi:10.1056/NEJMcp0910753
- Berbari EF, Kanj SS, Kowalski TJ, et al. 2015 Infectious Diseases Society of America (IDSA) Clinical Practice Guidelines for the Diagnosis and Treatment of Native Vertebral Osteomyelitis in Adults. Clin Infect Dis. Sep 15 2015;61(6):e26-46. PubMed PMID: 26229122. doi:10.1093/cid/civ482
- Chenoweth CE, Bassin BS, Mack MR, et al. Vertebral Osteomyelitis, Discitis, and Spinal Epidural Abscess in Adults. 2018. Michigan Medicine Clinical Care Guidelines.
- Johnson AJ, Zywiel MG, Stroh A, Marker DR, Mont MA. Serological markers can lead to false negative diagnoses of periprosthetic infections following total knee arthroplasty. Int Orthop. Nov 2011;35(11):1621-6. PubMed PMID: 21181540; PubMed Central PMCID: PMCPMC3193961. doi:10.1007/s00264-010-1175-5
- Dumas G, Joseph A, Zafrani L. Diagnostic tests for infections in critically ill immunocompromised patients. Intensive Care Med. Nov 2024;50(11):1920-1922. PubMed PMID: 39297946. doi:10.1007/s00134-024-07647-6
- Hall WA, Graeber A, Cecava ND. Vertebral Osteomyelitis. StatPearls. 2025.
- Alba-Loureiro TC, Munhoz CD, Martins JO, et al. Neutrophil function and metabolism in individuals with diabetes mellitus. Braz J Med Biol Res. Aug 2007;40(8):1037-44. PubMed PMID: 17665039. doi:10.1590/s0100-879×2006005000143
- Kawahigashi T, Harada Y, Watari T, et al. Missed Opportunities for Diagnosing Vertebral Osteomyelitis Caused by Influential Cognitive Biases. Am J Case Rep. Jun 22 2022;23:e936058. PubMed PMID: 35729859; PubMed Central PMCID: PMCPMC9238080. doi:10.12659/AJCR.936058
- Farouji A, Battah A, Hellou R, Ahmad A, Farouji I. Unique Presentation of Asymptomatic Bacteriuria, Vertebral Osteomyelitis, and Iliopsoas Abscess Due to Klebsiella pneumonia in a 73-Year-Old Man with Type 2 Diabetes Mellitus on Empagliflozin. Am J Case Rep. Jul 19 2024;25:e943874. PubMed PMID: 39026437; PubMed Central PMCID: PMCPMC11304661. doi:10.12659/AJCR.943874
Consent
Written informed consent was obtained from the patient for the publication of this case report, including all relevant clinical information and imaging. The patient reviewed the content and agreed to its publication in accordance with ethical standards.
Declarations/Disclosures
Funding/Conflicts of interest: In compliance with the ICMJE uniform disclosure form, author declares the following:
Payment/services info: Author has declared that no financial support was received from any organization for the submitted work.
Financial relationships: Author have declared that they have no financial relationships at present or within the previous three years with any organizations that might have an interest in the submitted work.
Other relationships: Author have declared that there are no other relationships or activities that could appear to have influenced the submitted work.