Author: Reham Alriyami MD *1, Mathew CL Phillips FRACP 2,3, Chris Giedt FRACP 1, Manjula Ratnaweera FRACP 1
Author Affiliation:
1 Department of Medicine, Waikato Hospital, Hamilton 3204, New Zealand.
2 Department of Neurology, Waikato Hospital, Hamilton 3204, New Zealand.
3 Department of Medicine, University of Auckland, Auckland 1142, New Zealand.
Competing Interests: The author/s declare no competing interests.
Issue: 15.01
DOI: 10.30756/ahmj.2025.15.01
Received: May 12, 2025
Accepted: Jun 12, 2025
Published: Jun 20, 2025
Recommended Citation: Alriyami R, Phillips MCL, Giedt C, Ratnaweera M. CGRP Shortened Recovery Period in Primary Cough Headache with Intravenous Metoclopramide: A Unique Case Report. Ann Head Med. 2025;15:01. DOI: 10.30756/ahmj.2025.15.01
Primary cough headache (PCH) is an uncommon condition characterized by a sudden burst of pain triggered by coughing or Valsalva maneuvers. It is considered “primary” in the absence of abnormalities in neuroimaging and cerebrospinal fluid (CSF) analysis. When an underlying abnormality is identified, the condition is termed “secondary cough headache.” The pathophysiology of primary cough headache is not fully understood, but it is thought to be related to increased intracranial pressure.
In terms of treatment, indomethacin is recommended for its effect on reducing intracranial pressure, despite the unclear mechanism of action. However, there is insufficient data to draw firm conclusions about the relative effectiveness of indomethacin. Alternatively, a growing body of theoretical evidence indicates that metoclopramide may also be an effective treatment for primary cough headache. Metoclopramide antagonizes dopamine D2 receptors as well as serotonin 5-HT3 receptors, both of which are strongly involved in mediating pain and nausea. Given this dual mechanistic influence, metoclopramide may potentially comprise an effective treatment for primary cough headache.
We reported a case of a typical primary cough headache in a male patient who showed favorable outcomes following intravenous metoclopramide, in combination with ibuprofen. The patient reported gradual improvement, with substantial recovery by day four and complete resolution by four weeks.
Abbreviations
PCH: Primary cough headache; CSF: Cerebrospinal fluid; D2: Dopamine receptor 2; 5-HT3: 5-hydroxytrypamine receptor 3; 5-HT4: 5-hydroxytrypamine receptor 4; CNS: Central nervous system; M2 muscarinic receptor 2; M4: Muscarinic receptor 4; COX: cyclooxygenase; IV: Intravenous.
Introduction
Headache triggered by coughing is an uncommon presentation and is typically classified into two types: primary and secondary.1, 2 Primary cough headache, previously known as benign cough headache or Valsalva maneuvers headache, is triggered by Valsalva maneuvers. These can include coughing, sneezing, laughing, straining, or stooping. Conversely, secondary cough headache, which accounts for about 40% of cough-induced headaches, is triggered by underlying brain pathology that causes increased intracranial pressure.1 The most common aetiologies of secondary cough headache include Chiari malformation type II and posterior fossa lesions. Secondary cough headaches are often accompanied by additional symptoms and neurological deficits, which vary depending on the underlying cause. 1, 2
Primary cough headache was initially considered an alarming symptom until Symonds and Rooke reported cases of benign cough headache. 1 It typically affects individuals over the age of 40, with the average age of onset around 60 years of age, and is more common in males than females.1 The pathophysiology is believed to be related to increased intracranial pressure caused by the rise in intra-abdominal and intrathoracic pressure during coughing. This leads to an increase in central venous pressure, which subsequently raises intracranial pressure. Several hypotheses have been proposed to explain this mechanism.1 Raskin hypothesized that pressure-sensitive receptors on the venous wall are activated by increased venous pressure. Another hypothesis suggests that systemic infections alter the vascular tone in cranial vessels, leading to headache. 1 Primary cough headache can be either unilateral or bilateral and is often described as a sharp, stabbing pain. The headache peaks immediately and typically lasts for one second to two hours. 3
Treatment strategies for primary cough headache are preventative and begin with reviewing the patient’s medications and changing or replacing whatever medication that causes cough. The preferred treatment is indomethacin, typically administered in therapeutic doses of 25 to 250 mg daily for at least 6 months. 1 Indomethacin works by reducing intracranial pressure, although there are no large randomized trials assessing its efficacy.2 Other pharmacological options include topiramate, methysergide, acetazolamide, propranolol, naproxen, and intravenous metoclopramide. 2 In some cases, cerebrospinal fluid drainage may be used to reduce intracranial pressure. 2
The prognosis of primary cough headache varies. Some cases have reported spontaneous remission, with the condition lasting anywhere from 1 to 42 months. The recurrence rate has been reported as 8.3%. 2
In this case report, we present a typical case of primary cough headache treated with intravenous metoclopramide and oral ibuprofen, which resulted in headache resolution within a shorter time frame than typically seen in the literature.
Case presentation
A 74-year-old New Zealand European man, fully independent and living with his wife, presented with an occipital headache radiating to the left hemicranium. During the two weeks prior, he had experienced a flu-like illness with a residual dry cough. This was followed by a headache, which came on suddenly, with coughing, sneezing, and stooping. The pain was described as shooting and intense (9/10 in severity) during coughing. The headache persisted until the patient took a combination tablet containing 500 mg paracetamol and 8 mg codeine phosphate, which provided only partial relief. There was no nausea, vomiting, photophobia, or phonophobia. There were no symptoms of neck rigidity, speech, swallowing, or hearing problems, and no sensory or motor deficits. He did not report any change in sensorium.
With respect to medical history, the patient had no history of neck pain or manipulation and had never experienced headaches before. He had a history of non-ST-elevation myocardial infarction four years prior, with coronary angiography showing left main stem disease, ostial left anterior descending artery disease, and right coronary artery disease, which was treated with coronary artery bypass grafting. This was associated with complications of post-sternotomy pain (due to broken sternotomy wires) and a post-bypass deep venous thrombosis. He also had a history of transient ischemic attack, type 2 diabetes, a resolved left diabetic partial abducens nerve palsy nine years ago, hypertension, dyslipidaemia, and benign prostate hyperplasia.
The patient had no history of smoking or alcohol use, and regular medications included vildagliptin, metformin, pioglitazone, aspirin, amlodipine, losartan, hydrochlorothiazide, metoprolol, ezetimibe, pravastatin, pantoprazole, and tamsulosin. He had documented allergies to trimethoprim/sulfamethoxazole (causing rash) and cotrimoxazole (causing Stevens-Johnson syndrome). He was also intolerant to atorvastatin (myalgia), empagliflozin, and dulaglutide (both causing gastrointestinal upset).
On examination, the patient was comfortable at rest but reported a distressing headache and mild nausea precipitated by coughing. He was afebrile, with a respiratory rate of 20 per min, blood pressure 130/80 mmHg, and oxygen saturations of 96% on room air. Cardiovascular exam revealed an ejection systolic murmur heard at the left sternal border. The chest was clear on auscultation, and the abdomen was soft and non-tender. On neurological exam, he was fully oriented. Cranial nerve exam was normal, including no papilledema and normal optic discs. All limbs showed normal tone, power, reflexes (2+ throughout), sensation, and coordination. Gait was normal. On laboratory investigations, the blood count, electrolytes, and inflammatory markers were all within normal ranges. A non-contrast computed tomography scan of the head showed small vessel disease, but no acute intracranial abnormalities. No other abnormalities were detected on magnetic resonance imaging of the brain, including magnetic resonance arteriography and venography. Cerebrospinal fluid analysis showed a normal opening pressure of 22 cm H2O, clear fluid, normal microscopy, and no xanthochromia, with a glucose level of 4.9 mmol/L and protein of 0.41 g/L.
The patient was admitted to our hospital under general medicine and continued to experience headaches triggered by coughing, sneezing, and stooping. He was treated with 10 mg of intravenous metoclopramide twice daily and 400 mg of oral ibuprofen twice daily for the first three days. Oral oxycodone immediate release 5 mg was also given, as well as a prophylactic laxative. The intensity of the headache gradually decreased from the third day onwards, and he felt comfortable enough to be discharged on day four of the admission. Follow-up was arranged, and the patient reported complete resolution of the headache after four weeks, coinciding with the resolution of his cough. The patient received oral oxycodone immediate release 5 mg during admission, but it was not continued after discharge. The resolution of his cough and headache occurred without ongoing opioid therapy. He did not experience any further Valsalva maneuver related headaches.
Discussion
This case presentation highlights the potential value of using metoclopramide in the management of primary cough headache. Although the precise mechanisms are complex, we suggest that the use of metoclopramide may be a promising treatment approach for primary cough headache, providing symptomatic relief in cases where other treatments may not be as effective.
When evaluating primary cough headache, it is essential to first determine the underlying cause of the cough before considering symptomatic treatment. Our patient had a history of complicated sternotomy, which might suggest increased intrathoracic pressure during coughing. However, this remains speculative, as the literature does not currently support a mechanical aetiology for primary cough headache. Although losartan has occasionally been implicated in cough, our patient had been on losartan for several years without issue, and his cough resolved while the medication was continued, making it an unlikely cause in this scenario. In this case, we concluded that his cough was most likely benign and post-viral in nature.
Indomethacin is generally the treatment of choice for primary cough headache. Although its mechanism of action is not fully understood, indomethacin is believed to work by decreasing intracranial pressure.1 It does not have an antitussive (cough-suppressing) effect. However, due to the limited number of comparative trials on the treatment of primary cough headache and the small sample sizes in many studies, there is no clear consensus on the superiority of indomethacin or any other treatment.1 Therefore, treatment tends to be individualized based on the patient’s needs and response.
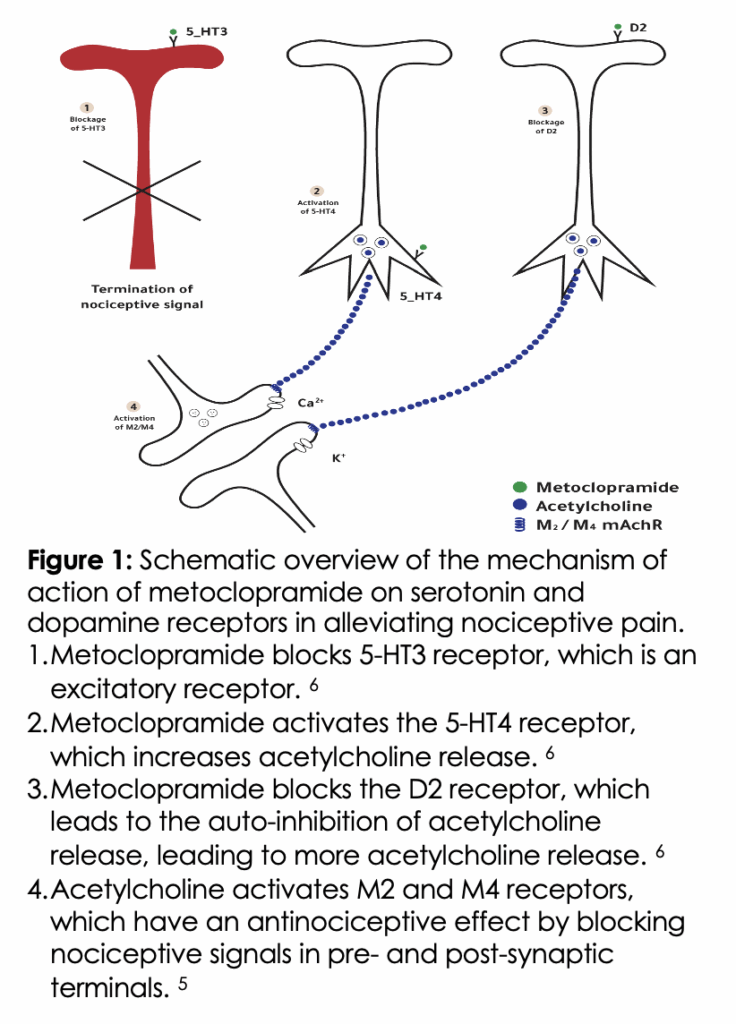
One potential therapeutic strategy in primary cough headache is to utilize a medication that combines antinociceptive, antiemetic, and antitussive properties. Metoclopramide is one such candidate, supported by preliminary clinical evidence. For example, in a study of patients presenting to the emergency department with cough-induced headaches secondary to viral tracheobronchitis, administration of 10 mg intravenous metoclopramide rapidly relieved pain within 1–2 hours.4 Metoclopramide is a D2 receptor antagonist, which explains its anti-emetic properties. This D2 antagonism also reduces hypersensitivity in the central nervous system, which helps alleviate pain. 4 Additionally, metoclopramide acts as a 5-HT3 receptor antagonist. 5 Most 5-HT3 receptors are located in areas of the CNS involved in pain and nausea modulation. 5 5-HT3 antagonists can alleviate vascular pain, especially in the context of inflammation and serotonin stimulation. 5 Moreover, metoclopramide may also stimulate 5-HT4 receptors located in nerve terminals, which, when activated, increase acetylcholine release. 6 Acetylcholine plays a role in analgesia, and its increased release may contribute to pain relief (see Figure 1 for the mechanism of action of metoclopramide on serotonin and dopamine receptors).
Furthermore, metoclopramide has been shown to promote the release of vasopressin, which is involved in vasomotor control and antinociception. 4 Vasopressin potentiates β-endorphin release from the anterior pituitary gland. B-endorphin appears to have morphine-like analgesic properties. The headache-aborting antinociceptive action of metoclopramide is linked to the stimulated release of vasopressin as well as an endogenous opiate, and its antitussive action is also likely linked to the release of an endogenous opiate, such as β-endorphin. 4
Notably, our patient was also treated with ibuprofen, which is a nonsteroidal anti-inflammatory drug. It is believed that ibuprofen works by inhibiting cyclooxygenase (COX), an enzyme involved in inflammation. There are at least two variants of cyclooxygenase (COX-1 and COX-2), and ibuprofen inhibits both. 7 The direct nociceptive effect of ibuprofen is achieved through COX-2 inhibition, which reduces the production of prostaglandins. 7 Prostaglandins lower the threshold for stimulation of nociceptive receptors. 7 The indirect mechanism involves activating the antinociceptive pathway by increasing the levels of the endocannabinoid anandamide, which in turn activates cannabinoid receptors in the central nervous system (CNS), thereby triggering the antinociceptive pathway. 7 In terms of efficacy, a clinical study involving ibuprofen, a randomized, double-blind, placebo-controlled study in acute migraine found that a metoclopramide + placebo group had significantly better relief of pain compared with an ibuprofen + placebo group. 8 Additionally, a systematic review comparing the safety and efficacy of metoclopramide to other anti-migraine medications, including ibuprofen, showed that a 10 mg IV metoclopramide was effective in relieving migraine attacks with minimal side effects. 9 However, to our knowledge, no trial has investigated the efficacy of ibuprofen for primary cough headache. Overall, given the relatively lower efficacy of ibuprofen in treating migraine combined with the fact that ibuprofen was only administered for 3 days in our patient, it most likely did not contribute a major role in the therapeutic effect.
Last, our patient was also treated with oxycodone, a semi-synthetic opioid agonist. 10 Oxycodone binds to the mu, kappa, and delta receptors in the central, peripheral, and autonomic nervous systems. 11 Its anti-nociceptive effect is primarily mediated by the kappa and mu receptors. 11 Although it is theoretically possible that oxycodone contributed to symptom relief, the patient received only a low dose (5 mg immediate-release) over a short period, and the medication was discontinued at discharge. Notably, his cough continued to improve and fully resolved over the following weeks, despite not receiving any further oxycodone. Therefore, while a minor antitussive effect cannot be entirely excluded, it is unlikely to have played a significant role in his clinical recovery.
Conclusion
Primary cough headache is characterized by a unilateral or bilateral severe, stabbing headache that is triggered by coughing or other Valsalva maneuvers. To date, no data support the superiority of one pharmacological treatment over another. This case provides insight into the potential effectiveness of utilizing metoclopramide as the primary agent for acute primary cough headache, which exhibits non-narcotic, antinociceptive, and antitussive properties. We hope this study will encourage further research into the efficacy of metoclopramide, as well as other agents, in its treatment.
References
- Cordenier A, De Hertogh W, De Keyser J, Versijpt J. Headache associated with cough: a review. J Headache Pain. May 20 2013;14(1):42. PubMed PMID: 23687906; PubMed Central PMCID: PMCPMC3671207. doi:10.1186/1129-2377-14-42
- Chen PK, Fuh JL, Wang SJ. Cough headache: a study of 83 consecutive patients. Cephalalgia. Oct 2009;29(10):1079-85. PubMed PMID: 19438909. doi:10.1111/j.1468-2982.2009.01844.x
- Olesen J. International Classification of Headache Disorders. Lancet Neurol. May 2018;17(5):396-397. PubMed PMID: 29550365. doi:10.1016/S1474-4422(18)30085-1
- Gupta VK. Metoclopramide aborts cough-induced headache and ameliorates cough–a pilot study. Int J Clin Pract. Feb 2007;61(2):345-8. PubMed PMID: 16787437. doi:10.1111/j.1742-1241.2006.00871.x
- Naser PV, Kuner R. Molecular, Cellular and Circuit Basis of Cholinergic Modulation of Pain. Neuroscience. Sep 1 2018;387:135-148. PubMed PMID: 28890048; PubMed Central PMCID: PMCPMC6150928. doi:10.1016/j.neuroscience.2017.08.049
- Heijmans L, Mons MR, Joosten EA. A systematic review on descending serotonergic projections and modulation of spinal nociception in chronic neuropathic pain and after spinal cord stimulation. Mol Pain. Jan-Dec 2021;17:17448069211043965. PubMed PMID: 34662215; PubMed Central PMCID: PMCPMC8527581. doi:10.1177/17448069211043965
- Mazaleuskaya LL, Theken KN, Gong L, et al. PharmGKB summary: ibuprofen pathways. Pharmacogenet Genomics. Feb 2015;25(2):96-106. PubMed PMID: 25502615; PubMed Central PMCID: PMCPMC4355401. doi:10.1097/FPC.0000000000000113
- Ellis GL, Delaney J, DeHart DA, Owens A. The efficacy of metoclopramide in the treatment of migraine headache. Ann Emerg Med. Feb 1993;22(2):191-5. PubMed PMID: 8427430. doi:10.1016/s0196-0644(05)80201-x
- Abdelmonem H, Abdelhay HM, Abdelwadoud GT, et al. The efficacy and safety of metoclopramide in relieving acute migraine attacks compared with other anti-migraine drugs: a systematic review and network meta-analysis of randomized controlled trials. BMC Neurol. Jun 8 2023;23(1):221. PubMed PMID: 37291500; PubMed Central PMCID: PMCPMC10249175. doi:10.1186/s12883-023-03259-7
- Ordonez Gallego A, Gonzalez Baron M, Espinosa Arranz E. Oxycodone: a pharmacological and clinical review. Clin Transl Oncol. May 2007;9(5):298-307. PubMed PMID: 17525040. doi:10.1007/s12094-007-0057-9
- Ross FB, Smith MT. The intrinsic antinociceptive effects of oxycodone appear to be kappa-opioid receptor mediated. Pain. Nov 1997;73(2):151-157. PubMed PMID: 9415500. doi:10.1016/S0304-3959(97)00093-6
Acknowledgments
We thank all the nurses, radiographers, and radiologists at Waikato Hospital for their participation in patient care.
Consent
An assigned consent form was obtained from the patient for publication
Declarations/Disclosures
Funding/Conflicts of interest: In compliance with the ICMJE uniform disclosure form, author declares the following:
Payment/services info: Author has declared that no financial support was received from any organization for the submitted work.
Financial relationships: Author have declared that they have no financial relationships at present or within the previous three years with any organizations that might have an interest in the submitted work.
Other relationships: Author have declared that there are no other relationships or activities that could appear to have influenced the submitted work.